Chapter: Modern Medical Toxicology: Neurotoxic Poisons: Inebriants
Ethanol: Clinical Features - Inebriant Neurotoxic Poisons
Clinical Features
Acute Poisoning (Intoxication,
Inebriation):
·
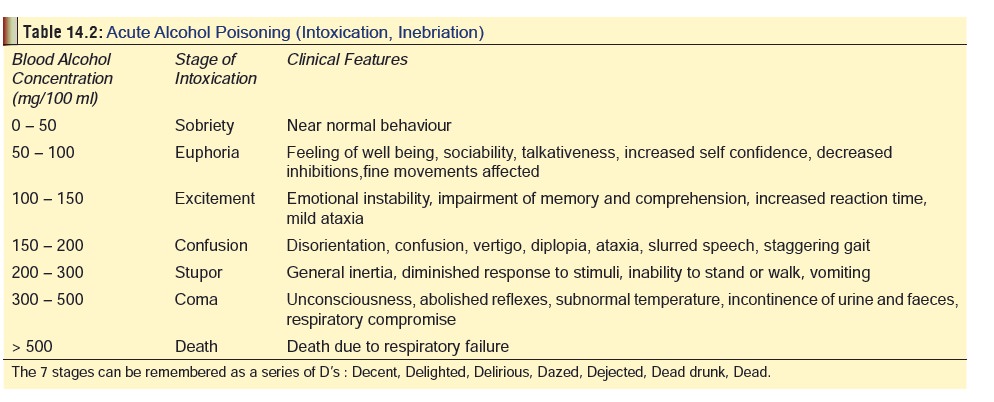
Initially, ethanol produces
excitement which progresses to loss of restraint, behavioural changes,
garrulous-ness, slurred speech, ataxia, unsteady gait, drowsiness, stupor, and
finally coma (Table 14.2).
·
Rarely, alcohol induces allergic reactions (usually in the
form of urticaria, nasal congestion, headache, etc.), which may be severe and
may even result in death.
·
There are also reports of cardiac dysrhythmias (espe-cially
atrial fibrillation) associated with binge drinking.
·
Through all the 7 stages of ethanol intoxication, a distinct
odour is perceptible in the breath of the indi-vidual. It is however not the
alcohol itself which imparts this odour but other nonalcoholic constituents
that give a particular flavour depending on the type of beverage consumed
(wine, beer, whisky, etc.). It is important to remember that even after a
person has completely sobered up from the effects of ethanol, the odour may
persist in the breath for a considerable period of time.
·
Ethanol is a mydriatic, but towards terminal stages (stages
of stupor and coma), the pupils may become constricted, only to dilate once
again at about the time of death. The McEwan
sign* is highly unreliable and
must not be depended upon for diagnosis of alcoholic coma.
·
Hypothermia is common.
·
Hypotension and tachycardia may be present. Atrial
fibrillation and atrioventricular block have been reported with acute overdose.
Cardiac output may be decreased in persons with pre-existing cardiac disease.
After consuming recreational amounts of alcohol, persons suffering from variant
angina may experience chest pain due to coronary artery spasm or myocardial
ischaemia. Sudden cardiac failure, arrhythmias, subclin-ical left ventricular
dysfunction, and other morphologic abnormalities of the heart can occur with
chronic heavy abuse. Alcoholic cardiomyopathy has insidious onset and can be
clinically inapparent. Symptoms of alco-holic cardiomyopathy are often present
for an average of 10–12 months before diagnosis, but as much as 85% of cases
have not been diagnosed through routine screening, unless angiography was
performed.
·
Bradypnoea may occur early, and tachypnoea may develop in
cases of metabolic acidosis.
·
Poor control of eye movements, with diplopia and nystagmus
may occur and alter vision and performance. Acute overdoses of ethanol have
caused spontaneous (not gaze-evoked) horizontal nystagmus. Amblyopia due to
peripheral neuritis has been reported in chronic alcoholics.
·
Bilaterally decreased vision occurs. Vitamin deficiencies
correlate with the ocular defects and early administration of B vitamins causes
recovery in some patients.
·
Lactic or ketoacidosis may occur. Acidosis may occur due to
metabolic disturbances, such as NADH over- production, oxidation of ethanol,
decreased lactate utilisation, and inhibition of hepatic gluconeogenesis.
Hypoglycaemia which can result in seizures and coma is a serious complication
of acute alcoholic intoxication, especially in children.
·
Medicolegally, stages 3 and 4 of alcoholic intoxication ![]() (stages of excitement and confusion) are the most
impor-tant, since most of the offences associated with drinking are committed
during these two stages. It is pertinent to mention that stage 7 (death) is
extremely rare in pure ethanol ingestion. In most cases there is recovery after
prolonged sleep, with some residual after effects (hang-over), consisting of headache, irritability, lethargy,
nausea,and abdominal discomfort. While the last mentioned is mainly due to
gastritis produced by ethanol, the other symptoms are actually the result of
congeners and impu-rities present in alcoholic beverages which cause mild
cerebral oedema. Part of the hangover may also be the result of hypoglycaemia
induced by ethanol.
(stages of excitement and confusion) are the most
impor-tant, since most of the offences associated with drinking are committed
during these two stages. It is pertinent to mention that stage 7 (death) is
extremely rare in pure ethanol ingestion. In most cases there is recovery after
prolonged sleep, with some residual after effects (hang-over), consisting of headache, irritability, lethargy,
nausea,and abdominal discomfort. While the last mentioned is mainly due to
gastritis produced by ethanol, the other symptoms are actually the result of
congeners and impu-rities present in alcoholic beverages which cause mild
cerebral oedema. Part of the hangover may also be the result of hypoglycaemia
induced by ethanol.
·
While the subject of some professional dispute, some data
indicate that a small number of people may be exceptionally sensitive to
ethanol, exhibiting combative and irrational behaviour after ingesting
non-intoxicating amounts. This has been termed pathological intoxica-tion or
ethanol idiosyncratic intoxication.
·
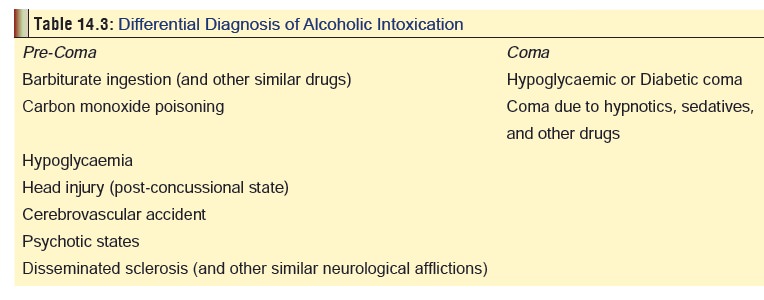
Alcoholic intoxication (through all
the stages) can mimic several conditions which can lead to errors in diagnosis.
Table 14.3 lists the differential
diagnosis for acute ethanol intoxication.
Related Topics