Chapter: Clinical Dermatology: Reactive erythemas and vasculitis
Erythema nodosum
Erythema
nodosum
Erythema
nodosum is an inflammation of the sub-cutaneous fat (a panniculitis). It is an
immunological reaction, elicited by various bacterial, viral and fungal
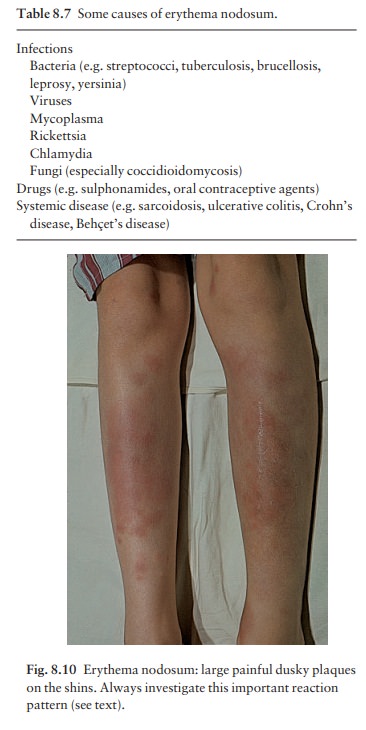
infections, malignant disorders, drugs and by a vari-ety of other causes (Table
8.7).
Presentation
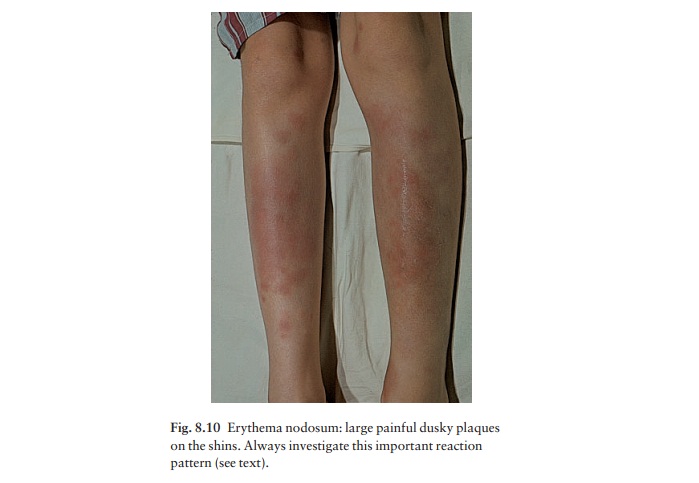
The characteristic lesion is a tender red nodule develop-ing alone or in groups on the legs and forearms or, rarely, on other areas such as the thighs, face, breasts or other areas where there is fat (Fig. 8.10). Some patients also have painful joints and fever.
Course
Lesions
usually resolve in 6–8 weeks. In the interim, lesions may enlarge and new ones
may occur at other sites. Like other reactive erythemas, erythema nodosum may
persist if its cause is not removed.
Complications
The
nodules may be so tender that walking is difficult. Erythema nodosum leprosum
occurs when lepromatous leprosy patients establish cell-mediated immunity to Mycobacterium
leprae. These patients have severemalaise, arthralgia and fever.
Differential diagnosis
The
differential diagnosis of a single tender red nodule is extensive and includes
trauma, infection (early cellulitis or abscess) and phlebitis.
When
lesions are multiple or bilateral, infection becomes less likely unless the
lesions are developing in a sporotrichoid manner. Other causes of a nodular
panniculitis, which may appear like erythema nodosum, include panniculitis from
pancreatitis, cold, trauma, injection of drugs or other foreign substances,
withdrawal from systemic steroids, lupus erythem-atosus, superficial migratory
thrombophlebitis, pol-yarteritis nodosa and a deficiency of α1-antitrypsin.
Some people use the term nodular vasculitis to describe a condition like
erythema nodosum that lasts for more than 6 months.
Investigations
Erythema
nodosum demands a careful history, physical examination, a chest X-ray, throat
culture for strepto-coccus, a Mantoux test and an antistreptolysin-O (ASO)
titre. If the results are normal, and there are no symptoms or physical
findings to suggest other causes, extensive investigations can be deferred
because the disease will usually resolve.
Treatment
The
ideal treatment for erythema nodosum is to iden-tify and eliminate its cause if
possible. For example, if culture or an ASO test confirms a streptococcal
infec-tion, a suitable antibiotic should be recommended. Bed rest is also an
important part of treatment. NSAIDs such as aspirin, indomethacin or ibuprofen
may be helpful. Systemic steroids are usually not needed. For reasons that are
not clear, potassium iodide in a dosage of 400 –900 mg/day can help, but should
not be used for longer than 6 months.
Whereas the reactive erythemas are associated with some inflammation around superficial or deep blood vessels, the term vasculitis is reserved for those showing inflammation within the vessel wall, with endothelial cell swelling, necrosis or fibrinoid change. The clinical manifestations depend upon the size of the blood vessel affected.
Related Topics