Chapter: Medical Electronics : Recent Trends in Medical Insrumentation
Endoscopy Unit
ENDOSCOPY UNIT
HISTORY
The first
endoscope, of a kind, was developed in 1806 by Philip Bozzini with his
introduction of a Lichtleiter (light conductor) for the examinations of the
canals and cavities of the human body. However, the Vienna Medical Society
disapproved of such curiosity. An endoscope was first introduced into a human
in 1822 by William Beaumont, an army surgeon at Mackinac Island, MichiganThe
use of electric light was a major step in the improvement of endoscopy. The
first such lights were external. Later, smaller bulbs became available making
internal light possible, for instance in a hysteroscope by Charles David in
1908Hans Christian Jacobaeus has been given credit for early endoscopic
explorations of the abdomen and the thorax with laparoscopy (1912) and
thoracoscopy (1910).Laparoscopy was used in the diagnosis of liver and
gallbladder disease by Heinz Kalk in the 1930. Hope reported in 1937 on the use
of laparoscopy to diagnose ectopic pregnancyIn 1944, Raoul Palmer placed his
patients in the Trendelenburg position after gaseous distention of the abdomen
and thus was able to reliably perform gynecologic laparoscopy
The first
gastrocamera was released in 1950 by Olympus Optical Co., Ltd. The device took
pictures on monochromatic film using a small light bulb that was triggered
manually. The device was of limited use, however, because it did not implement
real-time optical capability. Olympus continued its development of endoscopes
by incorporating fiber optics in the early 1960s, leading to the first useful
endoscopes. In 1964, it released a gastrocamera guided by a fiberscope. A
few articles claim that
Dr.Basil Hirschowitz of
Univ.Of M ichigan,Ann Arbor discussed the endoscope in early 50's.
As
endoscopic technolog y improved, so did the methods of gastroin testinal
endoscopy. Owing primarily to the efforts of Dr. Hiromi Shinya in the late
1960s, GI en doscopy developed into what is more recognizable a s today's
colonoscopy. While many doctors experimented with techniques to take advantage
of the new iterations of endoscopes, Dr. Shinya focused on techniques that
would allow for successful operation of the endoscope by an i ndividual,
rejecting the common practice at the time of utilizing two people.
Consequently, many of the fundamental methods and procedures of moderrn
colonoscopy were developed by Dr. Shinya.
By 1980,
laparoscopy tra ining was required by gynecologists to per form tubal ligation
procedures and diagnostic evalua tions of the pelvis. The first laparoscopic c
holecystectomy was performed in 1984 and the first video-laparoscopic
cholecystectomy in 1987. During the 1990s, laparoscopic surgery was extended to
the appendix, spleen, colon, stomach, kidney, and liver . Wireless capsule
endoscopy or C apsule Endoscopy is now approved in all the countries including
Japan where government reimb usement will be available from Oct.2007. Capsule
Endoscopy increases detection of Small Bowel tumors where traditional Endoscopy
is not very efficient.
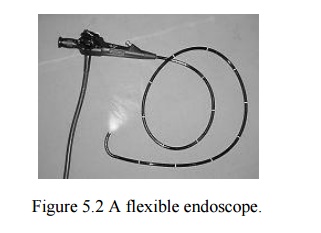
Endoscopy
An
endoscopy is a test that looks inside the body. The endoscope is a long flexible
tube that can be swallowed. It has a camera and light inside it. Some doctors
call it a telescope. Most likely to have an endoscopy to look at thhe inside of
Gullet
(oesophagus)
Stomach
Duodenum - the first part of the small bowel that attaches to the stomach
Large
bowel (colon)
There is
more detailed information about having a colonoscopy in the bowel cancer
section of Cancer Help UK. Below is information about having other types of
endoscopy.

Reflected
light rays are collected by CCD( Charge coupled device) and electrical
signals are produced, which are fed too the video monitor to get image. Thorough one channel of endoscope water and air is conducted to wash and dry the
surgical site. The endoscope also has a channel through which surgeons can
manipulate tiny instruments, such a s forceps, surgical scissors, and suction
devices.
A variety
of instruments can be fitted to the endoscope for different purposes.A surgeon
introduces the endoscope into thee body either through a body opening, such as
the mouth or the anus, or through a small incision in the skin.The endoscope
gives visual evidence of the problem, such as ulceration or inflammation It
can be used to collect a sample of tissue; remove problematic tissue, such as
polypss. It is used to take photograph of the hollow internal organs
Depending
on the body part, each type of endoscopy has its own special term, such as
laparoscopy
(abdo men, uterus, fallopian tube), laryngoscopy (vocal cords),
bronchoscopy
(lungs), colonoscopy (colo n), arthroscopy (joint) and Gastroscopy (Stom ach).
Components
An
endoscope can consist of
·
A rigid or flexible tube
·
A light delivery system to illuminate the organ or
object under inspection. The light source is normally outside the body and the
light is typically directed via an optical fiber system A lens system
transmitting the image to the viewer from the fiberscope
·
An additional channel to allow entry of medical
instruments or manipulators
Uses
Endoscopy
can involve
The
gastrointestinal tract (GI tract):
esophagus,
stomach and duodenum (esophagogastroduodenoscopy) small intestine
colon
(colonoscopy,proctosigmoidoscopy) Bile duct
·
The respiratory tract
·
The nose (rhinoscopy)
·
The lower respiratory tract (bronchoscopy)
· The urinary tract (cystoscopy)
·
The female reproductive system
·
The cervix (colposcopy)
·
The uterus (hysteroscopy)
·
The Fallopian tubes (Falloscopy)
·
Normally closed body cavities (through a small
incision):
· The abdominal or pelvic cavity (laparoscopy)
·
The interior of a joint (arthroscopy)
·
Organs of the chest (thoracoscopy and
mediastinoscopy)
·
During pregnancy
·
The amnion (amnioscopy)
·
The fetus (fetoscopy)
· Plastic Surgery
·
Panendoscopy (or triple endoscopy)
·
Combines laryngoscopy, esophagoscopy, and
bronchoscopy
Non-medical uses for endoscopy
The
planning and architectural community have found the endoscope useful for
pre-visualization of scale models of proposed buildings and cities
(architectural endoscopy) Internal inspection of complex technical systems
(borescope) Endoscopes are also a tool helpful in the examination of improvised
explosive devices by bomb disposal personnel. The FBI uses endoscopes for
conducting surveillance via tight spaces.
Risks
Infection
Punctured organs
Allergic
reactions due to Contrast agents or dyes (such as those used in a CT scan)
Over-sedation
After The Endoscopy
After the
procedure the patient w ill be observed and monitored by a qualified
individual in the endoscopy or a recovery area until a significant portion of
the medication has worn off. Occasionally a patient is left wit h a mild sore
throat, which promptly responds to saline gargles, or a feeling of distention
from the insufflated air that was used during t he procedure. Both problems are
mild and fleeting. When fully recovered, the patient will be instructed when to
resume his/her usual diet (probably within a few hours) and will be allowed to
be taken home. Because of the use of sedation, most facilities mandate that
the patient is taken home by another person and not to drive on his/her own or
handle machinery for the remainder of the day.
Recent developments
With the
application of robotic systems, telesurgery was introduced as the surgeon
could operate from a site physically removed fr om the patient. The first
transatlantic surgery has been called the Lindbergh Operation.
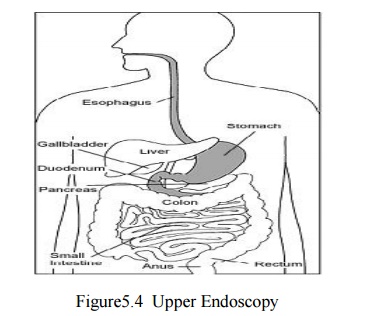
Upper Endoscopy
Upper
endoscopy enables the physician to look inside the esophagus, stomach, and
duodenum (first part of the small intestine ). The procedure might be used to
discover the reason for swallowing difficulties, nausea, vomiting, reflux,
bleeding, indigestion, abdominal pain, or chest pain. Upper endoscopy is also
called EGD, which stands for esophagogastroduodenoscopy
(eh-SAH-fuh-goh-GAS-troh-doo-AH-duh-NAH-skuh-pee).
For the
procedure you will swallow a thin, flexible, lighted tube called an endoscope
(EN-doh-skope). Right before the procedure the physician will spray your throat
with a numbing agent that may help prevent gagging. You may also receive pain
medicine and a sedative to help you relax during the exam. The endoscope
transmits an image of the inside of the esophagus, stomach, and duodenum, so
the physician can carefully examine the lining of these organs. The scope also
blows air into the stomach; this expands the folds of tissue and makes it
easier for the physician to examine the stomach.
The
physician can see abnormalities, like inflammation or bleeding, through the
endoscope that don't show up well on x rays. The physician can also insert
instruments into the scope to treat bleeding abnormalities or remove samples of
tissue (biopsy) for further tests.Possible complications of upper endoscopy
include bleeding and puncture of the stomach lining. However, such
complications are rare. Most people will probably have nothing more than a mild
sore throat after the procedure.The procedure takes 20 to 30 minutes. Because
you will be sedated, you will need to rest at the endoscopy facility for 1 to 2
hours until the medication wears off.
Preparation
Stomach
and duodenum must be empty for the procedure to be thorough and safe, will not
be able to eat or drink anything for at least 6 hours beforehand. Also, must
arrange for someone to take home—will not be allowed to drive because of the
sedatives. Physician may give other special instructions.
Need of Endoscopy
Endoscopy
allows physicians to peer through the body's passageways. Endoscopy is the
examination and inspection of the interior of body organs, joints or cavities
through an endoscope. An endoscope is a device that uses fiber optics and
powerful lens systems to provide lighting and visualization of the interior of
a joint. The portion of the endoscope inserted into the body may be rigid or
flexible, depending upon the medical procedure.
An
endoscope uses two fiber optic lines. A "light fiber" carries light
into the body cavity and an "image fiber" carries the image of the
body cavity back to the physician's viewing lens. There is also a separate port
to allow for administration of drugs, suction, and irrigation. This port may
also be used to introduce small folding instruments such as forceps, scissors,
brushes, snares and baskets for tissue excision (removal), sampling, or other
diagnostic and therapeutic work. Endoscopes may be used in conjunction with a
camera or video recorder to document images of the inside of the joint or
chronicle an endoscopic procedure. New endoscopes have digital capabilities for
manipulating and enhancing the video images.
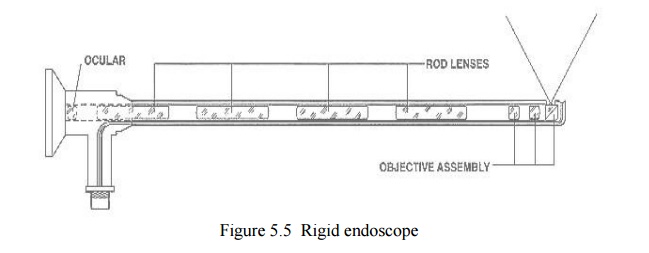
This
figure shows a rigid endoscope used for arthroscopy. The "image
fiber" leads from the ocular (eye piece) to the inserted end of the scope.
The "light fiber" is below and leads from the light source to the
working end of the endoscope.
Performance of Endoscopy
Endoscopy
can be used to diagnose various conditions by close examination of internal
organ and body structures. Endoscopy can also guide therapy and repair, such as
the removal of torn cartilage from the bearing surfaces of a joint. Biopsy
(tissue sampling for pathologic testing) may also be performed under endoscopic
guidance. Local or general anesthetic may be used during endoscopy, depending
upon the type of procedure being performed
Internal
abnormalities revealed through endoscopy include: abscesses, biliary (liver)
cirrhosis, bleeding, bronchitis, cancer, cysts, degenerative disease,
gallbladder stones, hernia, inflammation, metastatic cancer, polyps, tumors,
ulcers, and other diseases and conditions.
Endoscopy
is a minimally invasive procedure and carries with it certain minor risks
depending upon the type of procedure being performed. However, these risks are
typically far outweighed by the diagnostic and therapeutic potential of the
procedure.
Prior to
the widespread use of endoscopy and diagnostic imaging, most internal
conditions could only be diagnosed or treated with open surgery. Until the last
several decades, exploratory surgery was routinely performed only when a
patient was critically ill and the source of illness was not known. For
example, in certain dire cases, the patient's thorax or abdomen were surgically
opened and examined to try to determine the source of illness.
Endoscopy
can often be done on an outpatient basis. "Outpatient" means
that the procedure does not require hospital admission and acute care and
observation and may be performed outside the premises of a hospital. Outpatient
procedures performed at hospitals or ambulatory centers allow the patient to go
home or return to work within a short while after their procedure.
Types of Endoscopy
Fiber
optic endoscopes now have widespread use in medicine and guide a myriad of
diagnostic and therapeutic procedures including:
Arthroscopy: Examination of joints for
diagnosis and treatment (arthroscopic surgery)
Bronchoscopy: Examination of the trachea and
lung's bronchial trees to reveal abscesses,
bronchitis, carcinoma, tumors, tuberculosis, alveolitis, infection,
inflammation
Colonoscopy: Examination of the inside of the
colon and large intestine to detect polyps, tumors, ulceration, inflammation, colitis diverticula, Chrohn's disease,
and discovery and removal of foreign bodies.
Colposcopy: Direct visualization of the
vagina and cervix to detect cancer, inflammation, and other conditions.
Cystoscopy: Examination of the bladder,
urethra, urinary tract, uteral orifices, and prostate (men) with insertion of the endoscope through the urethra.
ERCP (endoscopic retrograde
cholangio-pancreatography) uses endoscopic guidance to place a catheter for x-ray fluorosocopy
with contrast enhancement. This technique is used to examine the liver's
biliary tree, the gallbladder, the pancreatic duct and other anatomy to check
for stones, other obstructions and disease. X-ray contrast is introduced into
these ducts via catheter and fluoroscopic x-ray images are taken to show any
abnormality or blockage. If disease is detected, it can sometimes be treated at
the same time or biopsy can be performed to test for cancer or other pathology.
ERCP can detect biliary cirrhosis,.cancer of the bile ducts, pancreatic cysts,
pseudocysts, pancreatic tumors, chronic pancreatitis and other conditions such
as gallbladder stones.
EGD (Esophogealgastroduodensoscopy): visual
examination of the upper gastro-intestinal (GI) tract. (also referred to as gastroscopy) to reveal hemorrhage,
hiatal hernia, inflammation of the esophagus, gastric ulcers.
Endoscopic biopsy is the
removal of tissue specimens for pathologic examination and analysis.
Gastroscopy: examination of the lining of the
esophagus, stomach, and duodenum. Gastroscopy is often used to diagnose ulcers and other sources of bleeding and
to guide biopsy of suspect GI cancers.
Laparoscopy: visualization of the stomach,
liver and other abdominal organs including the female reproductive organs, for example, the fallopian tubes.
Laryngoscopy: examination of the larynx (voice
box).
Proctoscopy, sigmoidoscopy,
proctosigmoidoscopy: examination of the rectum and sigmoid colon.
Thoracoscopy: examination of the pleura (sac
that covers the lungs), pleural spaces, mediastinum,
and pericardium.
Endoscopy Equipment
Endoscopes
have many practical needs. And H.M.B. Endoscopy Products (Hollywood, Florida)
has been providing endoscopic equipment and educating people on the use of
endoscopes for more than 17 years..
In the simplest
terms, Endoscopy equipment consists of instruments that can look at the inside
of many different organs — these are small, flexible or rigid tubes with a
light or lenses on the end that can look into the esophagus, stomach and colon
— and in more general terms endoscopy equipment can help doctors look deep
inside body structures and hollow organs. An endoscope and related endoscope
products and equipment are usually composed of three components:
An optic system that allows the doctor to look
through the scope into the organ or cavity, or to attach a video camera to the scope
A fiberoptic cable to light
up the bodily area
A lumen (e.g. the bore of a tube, like a
needle or catheter) to take tissue samples of the area being viewed
Related Topics