Chapter: Modern Medical Toxicology: General Principles: Diagnosis of Poisoning
Diagnosis of Poisoning
Diagnosis of Poisoning
A poisoning case can present to a
doctor or hospital in any one of a number of ways. Broadly, there are four types
of presentation:
· Fulminant—Produced by a massive dose. Death occursvery rapidly,
sometimes without preceding symptoms,
the patient appearing to collapse suddenly.
· Acute—Produced by a single dose or several small dosestaken in a
short period. Onset of symptoms is abrupt.
· Chronic—Produced by small doses taken over a longperiod. Onset is
insidious.
· Subacute—Characterised by a mixture of features of acuteand chronic
poisoning.
The majority of poisoned patients
presenting to the casualty (emergency) department are victims of acute
exposure. Most of them are usually coherent enough to tell the doctor what the
problem is, and indeed what they have taken or been exposed to. However, in an
unconscious or uncooperative patient the diagnosis will have to be made on the
basis of circumstantial or third party evidence. It is important to
inter-rogate the persons accompanying the patient (relatives, friends,
ambulance personnel, etc.), and to contact his or her family doctor as soon as
possible. In spite of all this, unfortunately, in a significant proportion of
cases the diagnosis remains uncertain. This is because unlike in other clinical
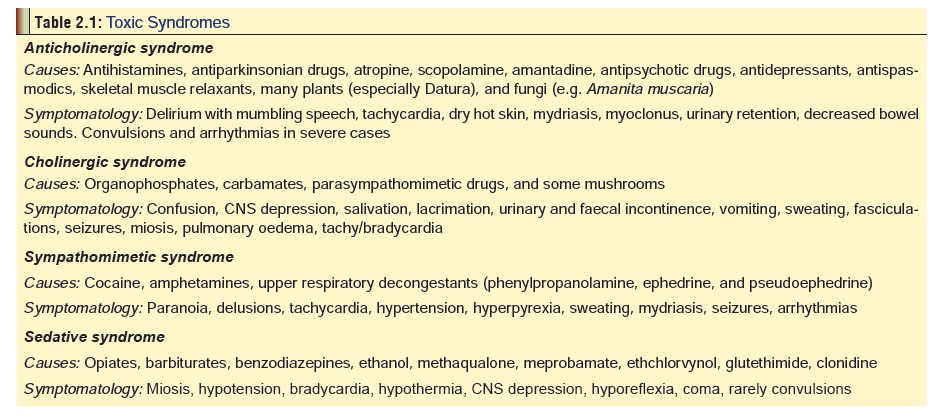
conditions arising out of natural disease, there are only a very few toxicsyndromes characterised by
specific signs and symptoms(Table 2.1).
In most cases, the poisoned patient presents with one or more of the following
non-specific features:
· Impairment of consciousness
· Respiratory/Cardiovascular
depression
· Dehydration due to
vomiting/diarrhoea
· Hypothermia
· Convulsions
· Cardiac arrhythmias
However, there are some valuable
clues afforded on detailed clinical examination which can help narrow down the
differen-tial diagnosis. Most of these will be dealt with in a subsequent
section (General Management), but a
few are discussed here for the sake of convenience.
·
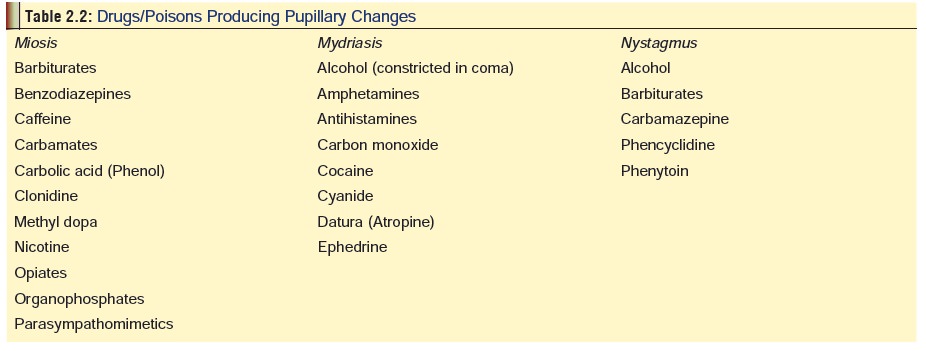
Ocular clues: Several drugs/poisons affect the
pupils of theeyes producing either miosis or mydriasis. A few produce
nystagmus. These have been laid out in Table
2.2. Normally, both the pupils are equal in size, 3 to 4 mm under typical
conditions, round, and react directly as well as consensu-ally to increased
light intensity by constricting.
Pupillary constriction also occurs
as part of the near reflex when a person focusses on near objects. All these
functions result from the balance between cholinergic innervation of the iris
sphincter (constrictor) by the oculomotor nerve, and sympathetic innervation of
the radial muscle of the iris (dilator). Mydriasis can occur due to increased
sympathetic stimulation by endogenous catecholamines or from systemic or ocular
exposures to sympathomimetic drugs. Mydriasis can also result from inhibition
of cholinergic mediated pupil-lary constriction. Because pupillary constriction
in response to light is a major determinant of pupil size, blindness from
ocular, retinal, or optic nerve disorders also leads to mydriasis. Pupillary
constriction or miosis can result from increased cholinergic stimulation, or
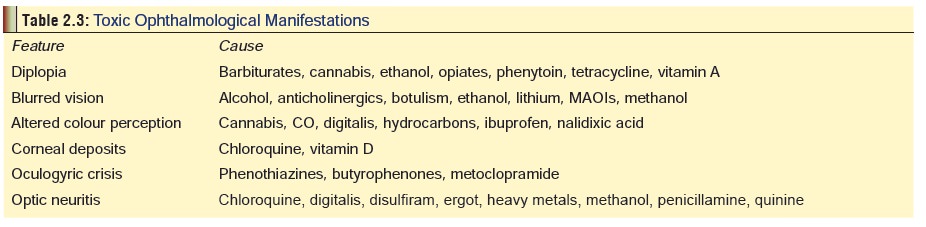
inhibition of sympa-thetic dilation. Other ophthalmological manifestations
along with their respective causes are mentioned in Table 2.3.
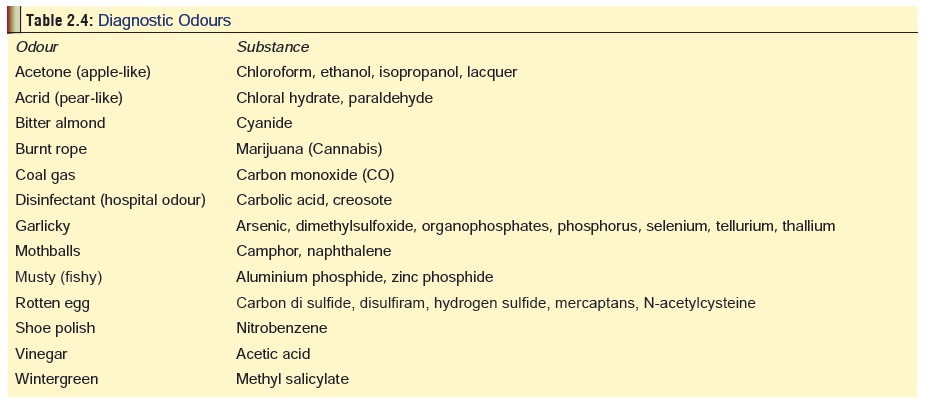
· Olfactory clues: Some poisons have distinctive
odourswhich may be perceived in the vicinity of a poisoned patient, especially
in the breath. Some important examples are mentioned in Table 2.4.
·
Dermal clues: Some poisons have characteristic
dermalmanifestations in acute toxicity, while certain others demonstrate skin
signs on chronic exposure (Table 2.5).
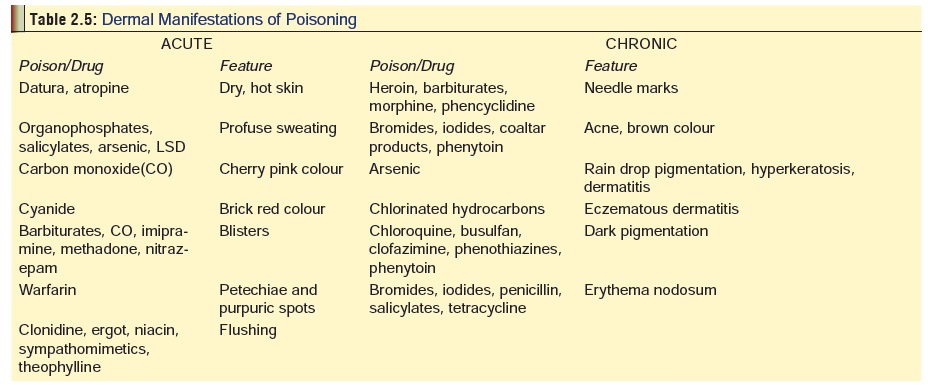
Several therapeutic drugs produce
irritant dermatitis even in non-toxic doses, e.g. most antibiotics, INH,
phenothiazines, sulfonamides, thiazides, NSAIDs, etc.
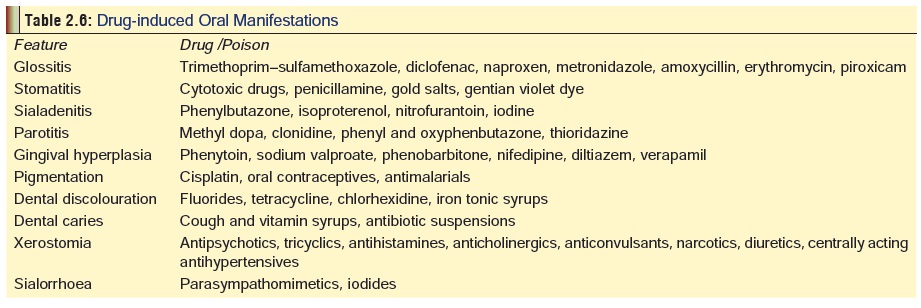
·
Oral clues: Careful examination of the mouth can
afford valuable information about the aetiology of poisoning in some cases
(Table 2.6).
Related Topics