Chapter: Pathology: Principles of Neoplasia
Diagnosis of Cancer
DIAGNOSIS OF CANCER
Histologic
diagnosis of cancer.Microscopic examination of tissue or
cells is requiredto make the diagnosis of cancer. Material suitable for
diagnosis of a tumor may be obtained by complete excision, biopsy, fine needle
aspiration, or cytologic smears (Pap test).
Immunohistochemistry may be
helpful in confirming the tissue of origin ofmetastatic or poorly
differentiated tumors. The technique uses monoclonal antibodies that are
specific for a cellular component. Among the many anti-bodies that are
clinically useful are:
·
All of the serum tumor markers
·
Thyroglobulin (thyroid cancers)
·
S100 (melanoma and neural tumors)
·
Actin (smooth and skeletal muscle)
·
CD markers (lymphomas/leukemias)
·
Estrogen receptors (breast cancer)
·
Intermediate filaments
Ancillary tests for the
diagnosis of cancer include electron microscopy, flowcytometry, cytogenetics,
and PCR/DNA probes.
Serum
tumor markers.Tumor markers are usually normal cellular components thatare
increased in neoplasms but may also be elevated in nonneoplastic conditions.
Serum tumor markers are used for screening (e.g., prostate specific antigen
[PSA]) for cancer, monitoring treatment efficacy, and detecting recurrence of
cancers.
·
Clinically
useful tumor markers include alpha-fetoprotein (AFP, used
forhepatoma, nonseminomatous testicular germ cell tumors); beta human
cho-rionic gonadotropin (hCG, used for trophoblastic tumors, choriocarcinoma);
calcitonin (used for medullary carcinoma of the thyroid); carcinoembryonic
antigen (CEA, used for carcinomas of the lung, pancreas, stomach, breast, and
colon); CA-125 (used for malignant ovarian epithelial tumors); CA19-9 (used for
malignant pancreatic adenocarcinoma); placental alkaline phosphatase (used for
seminoma); and prostate specific antigen (PSA, used for prostate cancer).
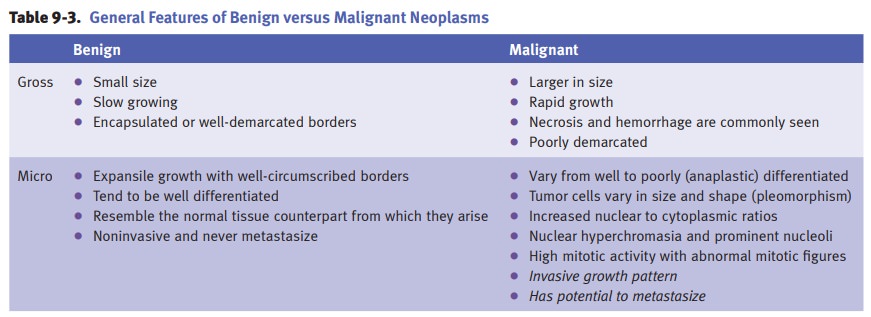
Grading
and staging. Tumor grade is a histologic estimate of the malignancy ofa
tumor, and typically uses criteria such as the degree of differentiation from
low grade (well-differentiated) to high grade (poorly
differentiated/anaplastic) and the number of mitoses.
Tumor
stage is a clinical estimate of the extent of tumor spread. TNM staging system
criteria is used for most tumor types:
·
T
indicates the size of the primary tumor.
·
N
indicates extent of regional lymph node spread.
·
M
indicates the presence or absence of metastatic disease.
In
general, staging is a better predictor of prognosis than tumor grade.
Tumor
progression refers to the tendency of a tumor to become more
malignantover time. This progression can be related to both natural selection
(evolution of a more malignant clone over time due to a selective growth
advantage) and genetic instability (malignant cells are more prone to mutate
and accumulate additional genetic defects).
Metastasis.Lymphatic spread is the most common initial route of spread for epi-thelial carcinomas. Early hematogenous spread is typically seen with most sarcomas (e.g., osteogenic sarcoma), renal cell carcinoma (because of the proximity of the large renal vein), hepatocellular carcinoma (because of the presence of the hepatic sinusoids), follicular carcinoma of the thyroid, and choriocarcinoma (because of its propensity to seek vessels). Seeding of body cavities and surfaces occurs in ovarian carcinoma. Transplantation via mechanical manipulation (e.g., surgical incision, needle tracts) may occur but is relatively rare.