Chapter: Medical Physiology: Regulation of Extracellular Fluid Osmolarity and Sodium Concentration
Countercurrent Mechanism Produces a Hyperosmotic Renal Medullary Interstitium
Countercurrent Mechanism Produces a Hyperosmotic Renal Medullary Interstitium
The osmolarity of interstitial fluid in almost all parts of the body is about 300 mOsm/L, which is similar to the plasma osmolarity. (thecorrected osmolar activity, which accounts for intermolecular attraction and repulsion, is about 282 mOsm/L.) The osmolarity of the interstitial fluid in the medulla of the kidney is much higher, increas-ing progressively to about 1200 to 1400 mOsm/L in the pelvic tip of the medulla. This means that the renal medullary interstitium has accumulated solutes in great excess of water. Once the high solute concentra-tion in the medulla is achieved, it is maintained by a balanced inflow and outflow of solutes and water in the medulla.
The major factors that contribute to the buildup of solute concentration into the renal medulla are as follows:
1. Active transport of sodium ions and co-transport of potassium, chloride, and other ions out of the thick portion of the ascending limb of the loop of Henle into the medullary interstitium.
2. Active transport of ions from the collecting ducts into the medullary interstitium
3. Facilitated diffusion of large amounts of urea from the inner medullary collecting ducts into the medullary interstitium
4. Diffusion of only small amounts of water from the medullary tubules into the medullary interstitium, far less than the reabsorption of solutes into the medullary interstitium
Special Characteristics of Loop of Henle That Cause Solutes to Be Trapped in the Renal Medulla. The transport character-istics of the loops of Henle are summarized in Table 28–1, along with the characteristics of the proximal tubules, distal tubules, cortical collecting tubules, and inner medullary collecting ducts.
The most important cause of the high medullary osmolarity is active transport of sodium and co-transport of potassium, chloride, and other ions from the thick ascending loop of Henle into the interstitium. This pump is capable of establishing about a 200-milliosmole concentration gradient between the tubular lumen and the interstitial fluid. Because the thick ascending limb is virtually impermeable to water, the solutes pumped out are not followed by osmotic flow of water into the interstitium. Thus, the active transport of sodium and other ions out of the thick ascending loop adds solutes in excess of water to the renal medullary interstitium. There is some passive reabsorption of sodium chloride from the thin ascend-ing limb of Henle’s loop, which is also impermeable to water, adding further to the high solute concentration of the renal medullary interstitium.
The descending limb of Henle’s loop, in contrast to the ascending limb, is very permeable to water, and the tubular fluid osmolarity quickly becomes equal to the renal medullary osmolarity. Therefore, water diffuses out of the descending limb of Henle’s loop into the interstitium, and the tubular fluid osmolarity gradually rises as it flows toward the tip of the loop of Henle.
Steps Involved in Causing Hyperosmotic Renal Medullary Inter-stitium. With these characteristics of the loop of Henlein mind, let us now discuss how the renal medulla becomes hyperosmotic. First, assume that the loop of Henle is filled with fluid with a concentration of 300 mOsm/L, the same as that leaving the proximal tubule (Figure 28–3, step 1).
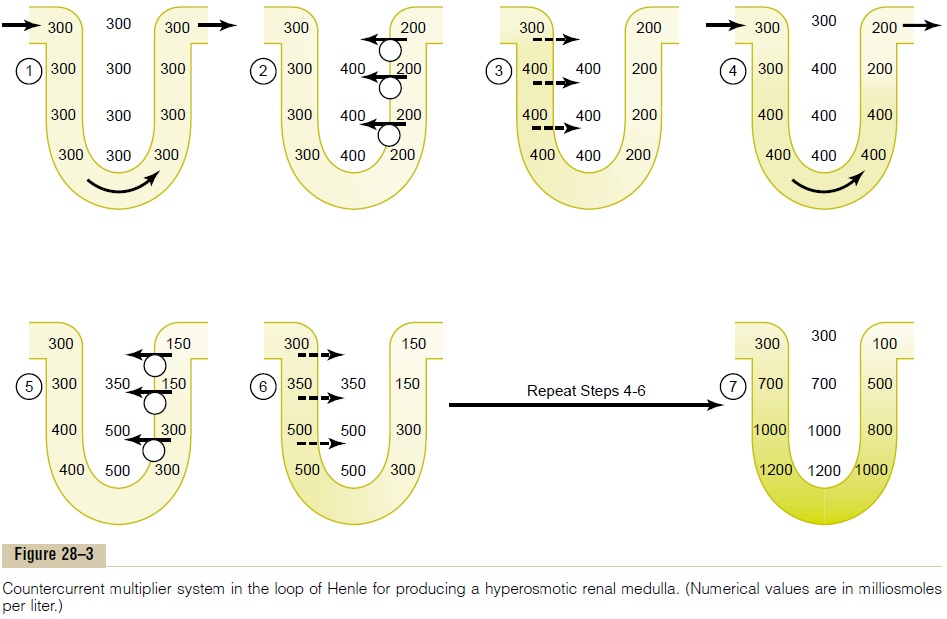
Next, the active pump of the thick ascending limb on the loop of Henle is turned on, reducing the concentration inside the tubule and raising the interstitial concentration; this pump establishes a 200-mOsm/L concentration gradient between the tubular fluid and the interstitial fluid (step 2). The limit to the gradient is about 200 mOsm/L because paracellular diffusion of ions back into the tubule eventually counterbalances transport of ions out of the lumen when the 200-mOsm/L concentration gradient is achieved.
Step 3 is that the tubular fluid in the descending limbof the loop of Henle and the interstitialfluid quicklyreach osmotic equilibrium because of osmosis of water out of the descending limb. The interstitial osmolarity is maintained at 400 mOsm/L because of continued transport of ions out of the thick ascending loop of Henle. Thus, by itself, the active transport of sodium chloride out of the thick ascending limb is capable of establishing only a 200-mOsm/L concentration gradi-ent, much less than that achieved by the countercur-rent system.
Step 4 is additional flow of fluid into the loop of Henle from the proximal tubule, which causes the hyperosmotic fluid previously formed in the descend-ing limb to flow into the ascending limb. Once this fluid is in the ascending limb, additional ions are pumped into the interstitium, with water remaining behind, until a 200-mOsm/L osmotic gradient is established, with the interstitial fluid osmolarity rising to 500 mOsm/L (step 5). Then, once again, the fluid in the descending limb reaches equilibrium with the hyper-osmotic medullary interstitial fluid (step 6), and as the hyperosmotic tubular fluid from the descending limb of the loop of Henle flows into the ascending limb, still more solute is continuously pumped out of the tubules and deposited into the medullary interstitium.
These steps are repeated over and over, with the net effect of adding more and more solute to the medulla in excess of water; with sufficient time, this processgradually traps solutes in the medulla and multiplies the concentration gradient established by the active pumping of ions out of the thick ascending loop of Henle, eventually raising the interstitial fluid osmolar-ity to 1200 to 1400 mOsm/L as shown in step 7.
Thus, the repetitive reabsorption of sodium chloride by the thick ascending loop of Henle and continued inflow of new sodium chloride from the proximal tubule into the loop of Henle is called the countercur-rent multiplier. The sodium chloride reabsorbed fromthe ascending loop of Henle keeps adding to the newly arrived sodium chloride, thus “multiplying” its con-centration in the medullary interstitium.
Related Topics