Chapter: Essential Anesthesia From Science to Practice : Applied physiology and pharmacology : Anesthesia and the lung
Control of breathing
Control of breathing
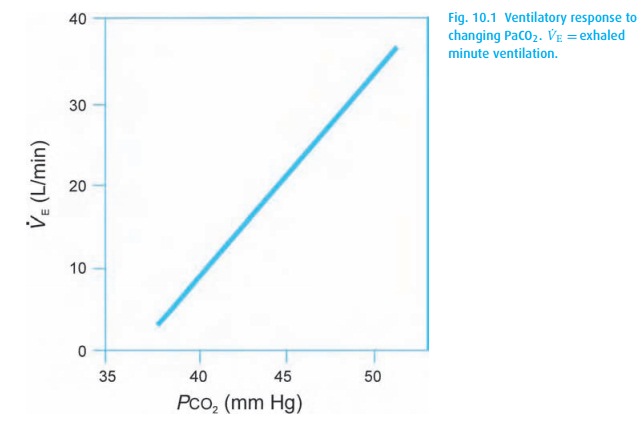
Can you commit suicide by simply not breathing or by willing your heart to stop? Even though we have voluntary muscular control over ventilation, we cannot stop breathing. We are hard-wired so that, in response to rising carbon dioxide tensions in the medulla, carbon dioxide-sensitive neurons stimulate ventilation to keep the arterial partial pressure of CO2 (PaCO2) near 40 mmHg. In physiological sleep, they let the PaCO2 drift up to 45 mmHg, while in pregnancy, they are reset by the controller to maintain 30 mmHg. Within physiological limits, ventilation and PaCO2 (Fig. 10.1) keep a linear relationship.
We can restrain the center pharmacologically with opioids or deep inhala-tion anesthesia. In some diseases resulting in high PaCO2, the respiratory center fatigues permanently, and these “CO2 retainers” must then rely on hypoxemia to drive their ventilation.
Perhaps surprisingly, oxygenation is not detected in the brain at all, but rather is sensed by peripheral chemoreceptors in the carotid and aortic bodies. These receptors do not really kick in until the PaO2 falls below about 60 mmHg. Thus, our “CO2-retaining” patients with chronic obstructive pulmonary disease (COPD) are not only chronically hypercarbic, they are also (at least borderline) hypoxemic. We often hear it said that such a patient will become apneic if given supplemental oxygen. Please do not take this to mean that, in an emergency, oxygen should be withheld from a hypoxemic patient for fear of apnea! Instead, give oxygen and ventilate the patient’s lungs. Once on top of the emergency, turn down the FiO2 step by step and remind the patient to breathe (no small task) until the oxygen saturation falls to a point where hypoxic drive takes effect. Similarly, when wean-ing these patients from mechanical ventilation, they might not start to breathe until returned to the hypoxic and hypercarbic state to which they are accustomed (another curse of smoking).
Related Topics