Chapter: Modern Pharmacology with Clinical Applications: Contemporary Drug Abuse
Contemporary Drug Abuse
Contemporary Drug Abuse
The phrases substance abuse and drug abuse are of-ten applied to the use of an illegal or illicit chemical substance (e.g., LSD,
heroin). However, these terms may be applied when a legally obtainable
medication is used excessively and for unintended purposes or is diverted to
someone else’s use. Also, some legal sub-stances (e.g., nicotine, alcohol) are
used to the detri-ment of the individual. Inappropriate use, or abuse, is the
excessive self-administration of any
substance for nonmedical purposes. An additional aspect of drug abuse is the
production of hazardous or harmful ef-fects to the individual and/or to
society. The etiology of substance abuse is a complicated phenomenon that is
sometimes a function of genetics, socioeconomic sta-tus, education, peer
pressure, thrill seeking, or experi-menting behavior and sometimes an
inappropriate at- tempt at self-medication
to treat a real or perceived disease state. It is also clear that drug abuse is
a func-tion of the pharmacology of each drug. Almost all abused substances
produce an effect on the brain that is perceived as desirable and will initiate
drug-seeking behavior.
The professionals in the drug
abuse field have such diverse backgrounds that adopting a common terminol-ogy
for terms such as addiction and dependence has been difficult. These
terms are best defined in the con-text of the pattern and consequences of drug
use. Regardless of the characteristics of the drug-induced in-toxication, the properties of the drug that are responsi-ble for
drug-seeking behavior are often referred to as the reinforcing properties. These drugs produce effects that are so
desirable that the user is compelled to obtain more of the drug.
Recurrent abuse of a drug may
properly be termed an addiction when
the individual becomes so obsessed with constantly obtaining and using a drug
that it be-comes a primary goal and disrupts the ability to func-tion in
family, social, or career settings. Typically, espe-cially during the initial
stages of drug addiction, the primary reinforcing property is the production of
eu-phoria, a term indicating anything
from happiness or pleasantness to an
excitement resembling sexual or-gasm. Euphoria is considered to be a positive reinforc-ing property, one that
the individual would desire or seek.
The evaluation of drugs for their reinforcing prop-erties is an assessment of
their abuse potential. The crav-ing
or desire to obtain additional drug, especially when it is not available, was
at one time termed psychological addiction or psychological dependence, though today these terms are not necessarily descriptive or specific. The term addiction should be used to describe
recurrent drug abuse, while the term dependence
(discussed later) refers to another state, a function of drug use, not drug
craving per se. Addiction has also
been used to describe recurrent substance abuse by individuals who realize it
is harmful to their health but cannot fulfill their desire to stop, such as
with tobacco.
Chronic use of a drug over a
long period sometimes produces a state of tolerance that may be classified as
pharmacokinetic, pharmacodynamic, or behavioral. The degree of tolerance is
generally proportional to the drug dose and the duration of use. In some cases,
partial or complete tolerance to the euphoric effect of the drug de-velops.
However, tolerance to many of the other acute effects also generally develops.
Termination of drug abuse may create a condition of drug abstinence, which coincides with the emergence of a measurable
physical syndrome. This abstinence syndrome
is an indication of dependence, is
often referred to as drug withdrawal, and was once termed physical dependence to distinguish it from psychological
dependence. It is assumed that adap-tation, or tolerance, to repeated
administration of drug is responsible for physical dependence. Generally, the
severity of the abstinence syndrome or level of depend-ence is proportional to
the degree of tolerance attained. However, the relationship between tolerance
and de-pendence has not been fully resolved; tolerance and dependence can occur
separately.
Epidemiological studies
indicate that most individu-als who abuse any one drug often also abuse, or
coabuse, other drugs during the same period. Polydrug abuse complicates
conclusions drawn from epidemio-logical and clinical studies. One reason for
coabuse of drugs relates to similarities in pharmacological effects. In these
cases, once tolerance to the primary drug de-velops, the individual also has cross-tolerance to related classes of
drugs. For example, the development of toler-ance to one CNS depressant, such
as barbiturates, anxi-olytic agents, or alcohol, simultaneously produces some
degree of tolerance to the other depressants. Users may attempt to ameliorate
selected drug effects by coabuse of drugs with opposite pharmacological
profiles.
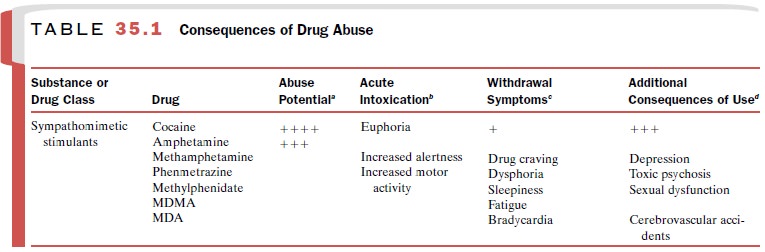
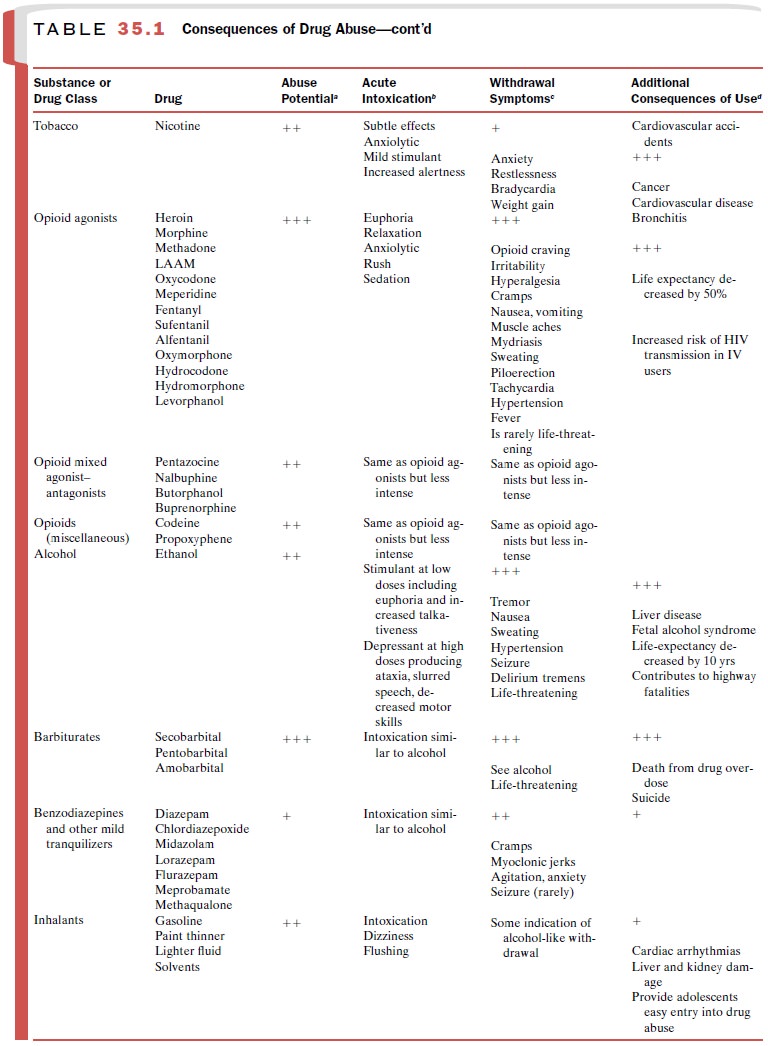
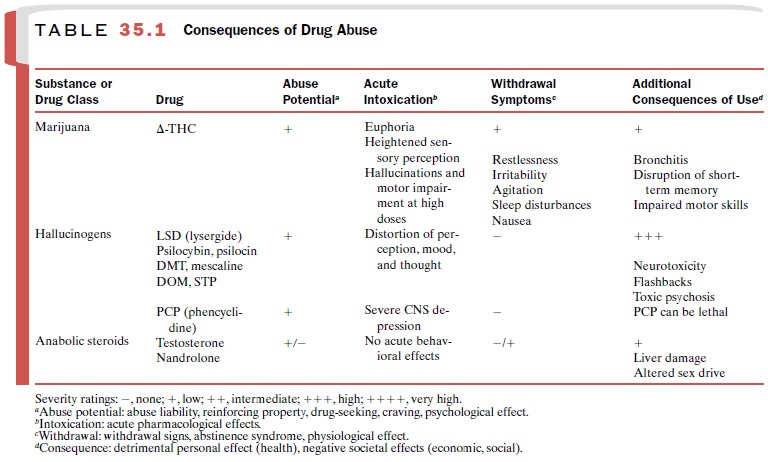
Drugs of abuse are derived
from numerous chemical classes, and therefore, it is not surprising that they
pro-duce distinctive pharmacological effects. Also, the con-sequences of acute
and chronic use vary considerably among different classes of compounds, as
summarized in Table 35.1.
Related Topics