Chapter: Ophthalmology: Eye Optics and Refractive Errors
Contact Lenses - Correction of Refractive Errors
Contact Lenses
Advantages and Characteristics of Contact Lenses
Contact lenses are in immediate contact with
the cornea. Although they are foreign bodies, most patients adapt to properly
fitted contact lenses. Contact lenses differ from eyeglasses in that they
correct the refractive error closer to the location of its origin. For this
reason, the quality of the optical
imageviewed through contact lenses is higher than that viewed through
eyeglasses.Contact lenses have significantly less influence on the size of
the retinal image than does correction with eyeglasses. Lenses do not cloud up
in rainy weather or steam, and peripheral distortion is minimized. The cosmetic
dis-advantage of thick eyeglasses in severe
ametropia is also eliminated. Severeanisometropia
requires correction with contact lenses for optical reasons, i.e.,to
minimize aniseikonia.
Contact lenses are defined by the following characteristics:
❖ Diameter of the contact lens.
❖ Radius of curvature of the posterior surface.
❖ Geometry of the posterior surface, i.e.,
spherical, aspherical, complex cur-vature, or toric.
❖ Refractive power.
❖ Material.
❖ Oxygen permeability of the material (Dk value).
The cornea requires oxygen from the precorneal
tear film. To ensure this supply, contact
lens materials must be oxygen-permeable. This becomes all the more
important the less the contact lens moves and permits circulation of tear
fluid. Contact lenses may be manufactured from rigid or flexible
materi-als.
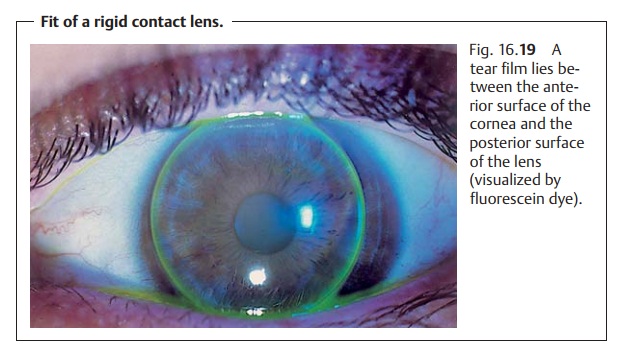
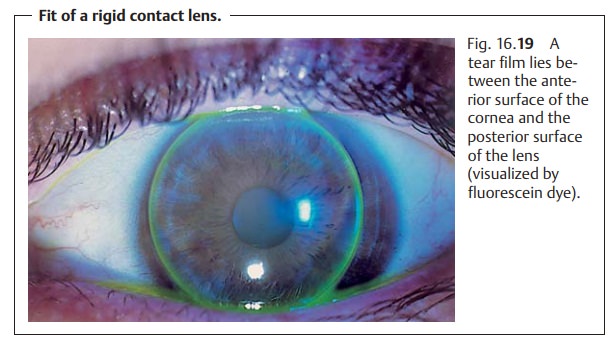
Rigid Contact Lenses
These contact lenses have a stable, nearly
unchanging shape. Patients takesome time
to become used to them and should therefore wear them often. Thegoal is to
achieve the best possible intimacy of fit between the posterior sur-face of the
lens and the anterior surface of the cornea (Fig. 16.19). This allows the contact lens to float on the precorneal tear
film. Every time the patient blinks, the lens is displaced superiorly and then
returns to its central position. This permits circulation of the tear film.
Previously, polymethyl methacrylate (PMMA) was used as a material.However, this is practically impermeable to oxygen. The lenses were fitted in small diameters with a very shallow curvature; the central area maintained contact with the cornea while the periphery projected. This allowed excellent tear film circulation, and patients were able to wear the lenses for surpris-ingly long periods. Today, highly oxygen-permeable materials such as silicone copolymers are available.
This eliminates the
time limit for daily wearing. These
lenses may also remain in the eye overnight in special cases, such as aphakic
patients with poor coordination (prolonged
wearing).
Rigid contact lenses can be manufactured as spherical lenses and toriclenses.Sphericalcontact lenses can almost completely
compensate forcor-neal astigmatism of less than 2.5 diopters. This is possible because the spacebetween
the posterior surface of the spherical contact lens and the anterior surface of
the astigmatic cornea is filled with tear fluid that forms a “tear lens.” Tear fluid has nearly the
same refractive index as the cornea. More
severe cor-neal astigmatism or
internal astigmatism requires correction with toric con-tact lenses. Rigid contact lenses can even correct
severe keratoconus.
Soft Contact Lenses
The material of the contact lens, such as
hydrogel, is soft and pliable. Patients find these lenses significantly more comfortable. The oxygen permeability of the material depends on its water content,
which may range from 36% to 85%. The higher the water content, the better the
oxygen permeability. However, it is typically lower than that of rigid
lenses. The material is more permeable to foreign substances, which can
accumulate in it. At 12.5 – 16 mm, flexible lenses are larger in diameter than
rigid lenses. Flexible lenses are often sup-ported by the limbus. The lens is
often displaced only a few tenths of a milli-meter when the patient blinks.
This greatly reduces the circulation of
tear filmunder the lenses. This limits the maximum daily period that patients are able towear them and
requires that they be removed at night to allow regeneration of the cornea.
Deviation from this principle is only possible in exceptional cases under the
strict supervision of a physician.
As the lenses are almost completely in contact
with the surface of the cor-nea, corneal
astigmatism cannot be corrected with spherical soft lenses. This requires
toric soft lenses.
Special Lenses
The following types of special lenses are
available for specific situations:
Therapeutic contact lenses:
In the presence ofcorneal
erosion,soft ultra-thin (0.05 mm) contact lenses act as a bandage and
thereby accelerate re-epithelialization of the cornea. They also reduce pain.
Soft contact lenses may also be used in patients receiving topical medication
as they store medication and only release it very slowly.
Corneal shields:
These are collagen devices that resemble contact lenses.These
shields are gradually broken down by the collagenase in the tear film. They are
used as bandages and substrates for topical medication in
the treat-ment of anterior disorders, such as erosion or ulcer.
Iris print lenses:
These colored contact lenses with a clear central pupil areused
in patients with aniridia and albinism.
They produce good cosmetic results, reduce
glare, and can correct a refractive error where indicated.
Bifocal contact lenses:
These lenses were developed to allow the use of con-tact lenses
in presbyopic patients. As in
eyeglasses, a near-field correction
is ground into the lens. This near-field portion is always located at the
bottom of the lens because the lens is heavier there. When the patient gazes
downward to read, the immobile lower eyelid pushes this near-field portion
superiorly where it aligns with the pupil and becomes optically effective.
Another possi-bility is diffraction
(bending of light rays as opposed to refraction) through concentric rings on
the posterior surface of the contact lens. This produces two images, a distant
refractive image and a near-field diffractive image. The patient chooses the
image that is important at the moment. It is also possible to correct one eye
for distance vision and the fellow eye for near vision (monocular vision).
Disadvantages of Contact Lenses
Contact lenses exert mechanical and metabolic
influences on the cornea.
Therefore, they require the constant supervision of an ophthalmologist.
Mechanical influences on the cornea can lead totransient
changes in refrac-tion. “Spectacle blur” can result when eyeglasses
suddenly no longer providethe proper correction after removing the lens.
Contact lenses require careful daily
cleaning and disinfection. This is more difficult, time-consuming, andmore
expensive than eyeglass care and is particular important with soft lenses.
Metabolic influences on the cornea:
The macromolecular mesh of materialabsorbs proteins, protein
breakdown products, low-molecular-weight sub-stances such as medications and
disinfectants, and bacteria and fungi. Serious complications can occur where
daily care of the contact lenses is inadequate. With their threshold oxygen
permeability, soft contact lenses interfere with corneal metabolism. Contact
lenses are less suitable for patients with symp-toms of keratoconjunctivitis
sicca.
Contact Lens Complications
Complications have been observed primarily in
patients wearing soft contact lenses.
These include:
Infectious keratitis (corneal infiltrations and ulcers) caused by bacteria,fungi, and
protozoans.
Acanthamoeba keratitis is a serious complication affecting wearers ofsoft
contact lenses and often requires penetrating keratoplasty.
Giant papillary conjunctivitis:
This is an allergic reaction of the palpebralconjunctiva of the
upper eyelid to denatured proteins. It results in prolifera-tive “cobblestone”
conjunctival lesions.
Corneal vascularization may be interpreted as the result of insufficientsupply of oxygen
to the cornea.
Severe chronic conjunctivitis:
This usually makes it impossible to continuewearing contact
lenses.
Related Topics