Chapter: Medical Surgical Nursing: Management of Patients With Immunodeficiency
Combined B-Cell and T-Cell Deficiencies
COMBINED
B-CELL AND T-CELL DEFICIENCIES
Pathophysiology
Combined B-cell and T-cell deficiencies are
those disorders of the immune system that have elements of dysfunction of both
the B cells and T cells. A variety of inherited (autosomal recessive and
X-linked) conditions fit this description. These conditions have in common
disruption of the normal communication system of B cells and T cells and
impairment of the immune response (Porth, 2002). These conditions generally
appear early in life. Ex-amples of these deficiencies are discussed below.
Ataxia-telangiectasia is an autosomal recessive disorder af-fecting both T- and B-cell
immunity. In 40% of patients with this disease, a selective IgA deficiency
exists. IgA and IgG subclass deficiencies, along with IgE deficiencies, have
been identified. Variable degrees of T-cell deficiencies are observed and
become more severe with advancing age. The disease is associated with
neurologic, vascular, endocrine, hepatic, and cutaneous abnor-malities. It is
accompanied by progressive cerebellar ataxia, telangi-ectasias, recurrent
bacterial infection of the sinuses and lungs, and an increased incidence of
cancer (Buckley, 2000).
Both B
and T cells are missing in severe
combined immuno-deficiency disease (SCID). SCID is a phenotypic term that
isused for a wide variety of congenital and hereditary immunologic defects that
are characterized by early onset of infections, defects in both B- and T-cell
systems, lymphoid aplasia, and thymic dys-plasia. Inheritance of this disorder
can be X-linked, autosomal-recessive, or sporadic. The exact incidence of SCID
is unknown; it is recognized as a rare disease in most population groups, with
an incidence of about 1 case in 1,000,000. This illness occurs in all racial
groups and both genders (Parslow et al., 2001). Wiskott-Aldrich syndrome is a variation of SCID compoundedby
thrombocytopenia (loss of platelets). The prognosis is gener-ally poor because
most affected infants develop overwhelming fatal infections.
Clinical Manifestations
The onset of ataxia (uncoordinated muscle movement) telangi-ectasia (vascular lesions caused by dilated blood vessels)
usually oc-curs in the first 4 years of life of those with ataxia-telangiectasia.
Many patients, however, remain symptom-free for 10 years or longer. As patients
approach the second decade of life, chronic lung disease, mental retardation,
neurologic symptoms, and physical disability become severe. Long-term survivors
develop progressive deterioration of immunologic and neurologic func-tions.
Some affected patients have reached the fifth decade of life. The primary
causes of death in these patients are overwhelming infection and
lymphoreticular or epithelial cancer.
The onset of symptoms occurs within the first
3 months of life in the majority of patients with SCID with respiratory
infections, pneumonia (often secondary to P.
carinii), thrush, diarrhea, and failure to thrive. Many of these infections
are resistant to treat-ment. Shedding of viruses such as respiratory syncytial
virus or cytomegalovirus from the respiratory and gastrointestinal tracts is
persistent. Maculopapular and erythematous skin rashes may occur. Vomiting,
fever, and a persistent diaper rash are also com-mon manifestations (Parslow et
al., 2001).
Medical Management
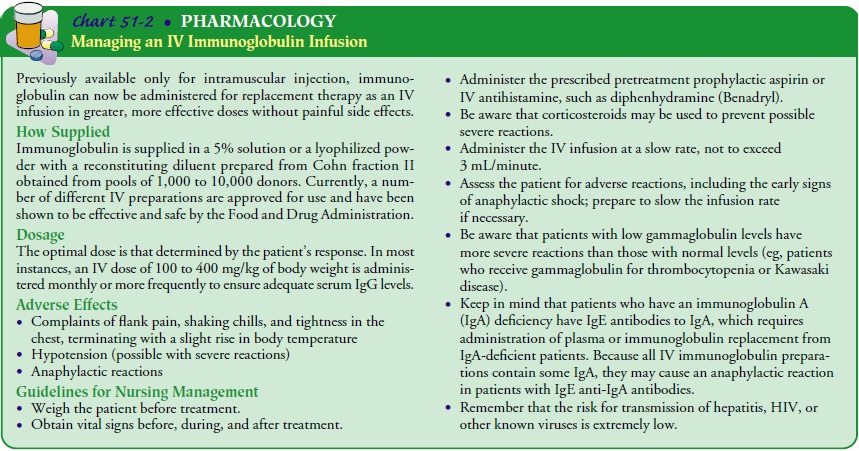
Treatment of ataxia-telangiectasia includes
early management of infections with antimicrobial therapy, management of
chronic lung disease with postural drainage and physical therapy, and management
of other presenting symptoms. Other treatments in-clude transplantation of
fetal thymus tissue and IVIG adminis-tration (Chart 51-2).
Treatment
options for SCID include stem cell and bone marrow transplantation. The ideal
donor is an HLA-identical sibling (Parslow et al., 2001). Other treatment
regimens include IVIG replacement, administration of thymus-derived factors,
and thymus gland transplantation. Gene therapy has been used, but the results
have thus far been disappointing. As treatment im-proves, an increased number
of those who previously would have died in infancy may live to adulthood.
Nursing Management
As many patients require immunosuppression to
ensure engraft-ment of depleted bone marrow during certain transplantation
procedures, nursing care must be exquisite, with attention to pre-venting the
transmission of infection to patients. Use of standard precautions and
meticulous hand hygiene is essential in caring for these patients. Reverse
isolation procedures, where nurses pro-tect the patient by donning gowns,
gloves, caps, and so on, is essential. The patient’s condition must be
monitored at all times as a certain number of patients experience reactions to
transplan-tation that can be fatal.
Related Topics