Chapter: Microbiology and Immunology: Bacteriology: Streptococcus and Enterococcus
Clinical Syndromes - Streptococcus pyogenes
Clinical Syndromes
S. pyogenes produces a variety of clinical manifestations. These infections can be classified broadly as: (a) suppurative strepto-coccal diseases, (b) toxin-mediated disease, and (c) nonsuppura-tive streptococcal diseases.
◗ Suppurative streptococcal diseases
Respiratory infections
Pharyngitis: S. pyogenesis the most common bacteriumcausing pharyngitis or sore throat. Pharyngitis is characterized by inflammation of pharyngeal mucosa with exudate formation, tender enlarged cervical lymph nodes, fever, and leukocytosis. The condition is commonly seen in children and it spreads by droplet nuclei. The incubation period is 1–4 days. Uncomplicated pharyngitis resolves within 3–5 days.
Skin and soft tissue infections
Pyoderma: Pyoderma or impetigo is a localized infection of theskin, primarily affecting face, arms, legs, and other exposed parts of the body. The infection is acquired by direct contact with an infected person or fomites. The condition is caused by a limited number of serotypes (49, 53–55, 59–61, etc.) of S. pyogenes. The condition is seen mainly in young children. In tropics, impetigo is one of the important causes of acute glomerulonephritis (AGN) in children.
Erysipelas: Erysipelas is an acute and diffused infection ofthe skin, affecting the superficial lymphatics. It is characterized by red, swollen, and indurated skin with well-marked and raised borders. The affected skin is clearly demarcated from the surrounding healthy area. Commonly, face and legs are affected. Erysipelas occurs most commonly in young children or in older adults.
Cellulitis: Cellulitis is the infection of skin and subcutaneoustissues characterized by local inflammation like edema, erythema, tenderness, fever, headache, malaise, and other systemic manifestations. It is spreading in nature, often without any apparent focus of infection. The entry of the pathogen may be at a location distant to the lesion.
Necrotizing fasciitis: Necrotizing fasciitis occurs as a rapidlyspreading streptococcal infection of superficial and deep fascia. The infection is caused by certain M strains of S. pyogenes (M types 1 and 3), which produce pyrogenic exotoxins. These strains are also called as “flesh-eating strains” due to the extensive destruction of muscle and fascia caused by them. The condition is also associated with a toxic shock-like syndrome, leading to disseminated intravascular coagulation and multisystem failure.
Toxin-mediated diseases
Scarlet fever: Scarlet fever is a complication of streptococcalpharyngitis caused by certain strains of S. pyogenes producing pyrogenic exotoxins. It manifests as fever, pharyngitis, and by a characteristic rash. The rash is followed by desquamation. However, with the use of penicillin and other antibiotics, the suppurative complications of pharyngitis including scarlet fever have become rare.
Streptococcal toxic shock syndrome: Streptococcal toxicshock syndrome is caused by certain strains of S. pyogenes (M serotypes 1 or 3) that have prominent hyaluronic acid capsule. This is a condition similar to staphylococcal toxic shock syndrome. The condition manifests initially as pain at the site of inflammation and nonspecific systemic complaints, such as nausea, vomiting, diarrhea, fever, and chills. The condition progresses subsequently to multiorgan failure and shock. S. pyogenes is always isolated from the blood in toxic shock syndrome. The condition occurs in people of all ages. However, patients with HIV infection, varicella-zoster infection, diabetes, heart diseases, and intravenous drug and alcohol abusers are at high risk for streptococcal toxic shock syndrome.
Other suppurative streptococcal diseases
Other pyogenic infections caused by S. pyogenes include lym-phangitis, puerperal sepsis, abscesses of the internal organs (liver, lungs, kidneys, brain, etc.), and bacteremia.
◗ Nonsuppurative streptococcal diseases
Acute glomerulonephritis: AGN is a nonsuppurative compli-cation of S. pyogenes infection. The onset of infection typically occurs 2–3 weeks following skin infection or pharyngitis caused by certain pharyngeal (M types 1, 12) and pyodermal strains (M types 49, 53–55, 59–61) of S. pyogenes. M protein type 49 skin infection is most frequently implicated. The disease occurs as a result of deposition of antigen–antibody complexes on the glo-merular basement membrane, initiating inflammation. This leads to the manifestation of disease with hypertension, gen-eralized edema, hematuria, and proteinuria. It has an excellent prognosis, and most young patients usually recover completely.
Rheumatic fever: Rheumatic fever is an immunologicallymediated disease, which affects the heart, joints, skin, and brain. It has a latent period of 2–4 weeks. It is characterized by fever, migrating polyarthritis, and carditis, and is frequently associated with subcutaneous nodules. Damage to heart valves may occur during the course of infection.
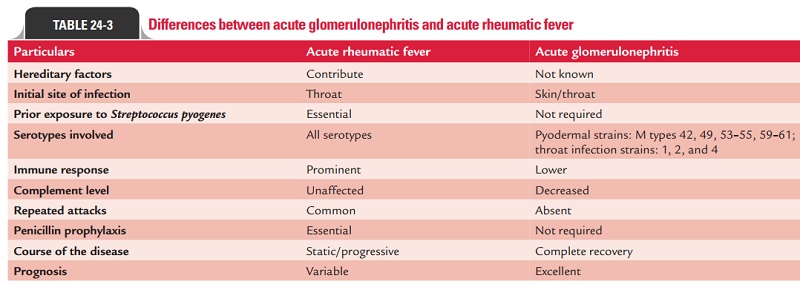
The comparison of AGN and rheumatic fever is presented in Table 24-3.
Related Topics