Chapter: Ophthalmology: Uveal Tract (Vascular pigmented layer)
Chronic Iritis and Iridocyclitis
Chronic Iritis and Iridocyclitis
Epidemiology:
About one quarter of alliridocyclitiscases have a chronicclinical course.
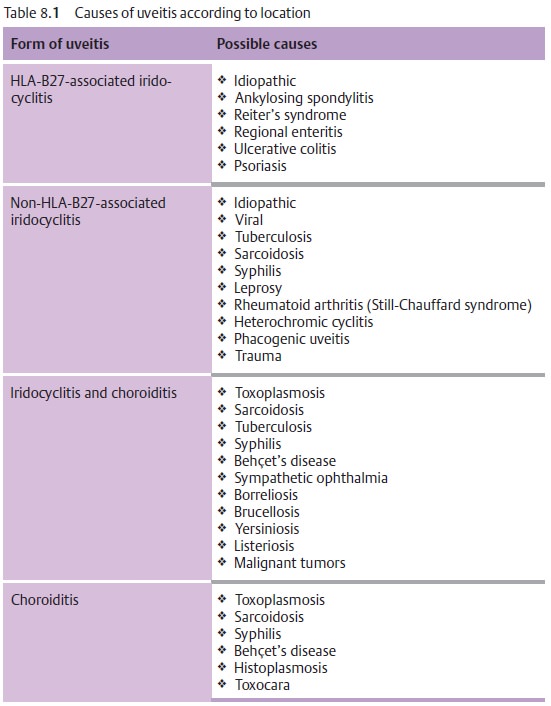
Etiology:
See Table 8.1.
Symptoms:
See acute iridocyclitis. Chronic iridocyclitis
may exhibit minimalsymptoms.
Diagnostic considerations:
See acute iridocyclitis.
Differential diagnosis:
The disorder should be distinguished from
acuteglaucoma, conjunctivitis, and keratitis.
Complications:
Total obliteration of the pupil by posterior synechiae
isreferred to a pupillary block.
Because the aqueous humor can no longer circu-late, secondary angle closure glaucoma with iris bombé occurs. Occlusion of the pupil also results in
fibrous scarring in the pupil. This can lead to thedevelopment of posterior
subcapsular opacities in the lens (secondary
cataract). Recurrent iridocyclitis can also lead to calcific band
keratopathy.
Treatment:
In pupillary
block with a secondary angle closure glaucoma, aNd:YAG laser iridotomy may be performed to create a shunt to allow
theaqueous humor from the posterior chamber to circulate into the anterior
chamber. In the presence of a secondary
cataract, a cataract extraction
may be performed when the inflammation has abated.
Prognosis:
Because of the chronic recurrent course of the
disorder, it frequently involves complications such as synechiae or cataract
that may progress to blindness from shrinkage of the eyeball.
Related Topics