Chapter: Case Study in Obstetrics and Gynaecology: Peripartum Care and Obstetric Emergencies
Case Study Reports: Labour
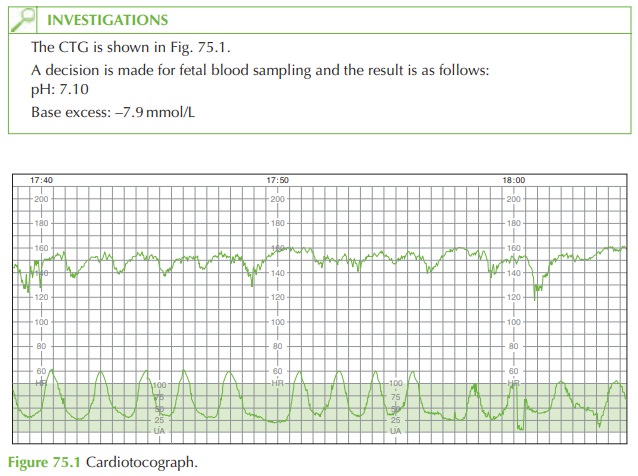
LABOUR
History
You are on the labour
ward and called
to see a 33-year-old woman
in labour as the mid- wife is concerned about the cardiotocograph (CTG).
She
is 41 + 2 weeks’ gestation and this is her first
baby. The pregnancy was
uncompli- cated until 2 days ago when she developed mild hypertension, without
proteinuria. In view of the gestational age a decision
was made for induction of labour yesterday. She had 2 mg prostaglandin gel
administered into the
vagina at 18.00
last night and
again at 06.00 this morning.
Spontaneous rupture of membranes occurred
at 10.00 today after which contractions commenced.
Examination
Blood pressure is 135/68 mmHg, heart
rate 90/min and temperature is 37.1°C.
On
abdominal palpation the
fetus is cephalic, 1/5 palpable, and
strong contractions are felt. Vaginally the cervix is fully effaced and 6 cm dilated. The fetus is cephalic at ischial
spines with mild caput but no moulding.
Grade 1 meconium is noted.
Questions
·
How
would you interpret
the CTG and fetal blood sample result?
·
How would you manage the patient?
Answer:
The
CTG shows a baseline of 155 beats/min with reduced variability (5–10 beats/min) and late decelerations. No accelerations are seen. The CTG is therefore classified as abnormal.
Contractions are 5 in 10.

The
fetal pH should
normally be between
7.25 and 7.35.
This fetal blood
sample suggests an acidotic
baby (low pH and high negative base excess).
In
cases of an abnormal CTG,
the fetus may
not be compromised, and it is therefore
important to assess the fetal
wellbeing with a fetal blood
sample before progressing to operative intervention (unless
fetal blood sampling
is contraindicated or in cases
of per- sistent fetal
bradycardia). In this case the fetal blood
sample confirmed that the fetus
was significantly compromised.
The
meconium-stained liquor may
be a sign of fetal
compromise, but at 41 weeks’ gesta- tion meconium may be an incidental finding and is therefore difficult to interpret.
Management
If
the cervix were fully dilated
and the head below the ischial spines
then instrumental delivery, by ventouse or forceps, would
be appropriate. As this is not the
case, then imme- diate delivery by Caesarean section is essential. The important points
for an emergency Caesarean section
are:
·
the midwife in charge, theatre
staff, obstetric consultant, specialist registrar, anaesthetist and
paediatrician should be informed
·
the
reasons for the proposed procedure
should be explained
to the woman and informed
consent obtained
·
metoclopramide and ranitidine should
be given in case of the need for general anaesthetic
·
intravenous access is needed
with full blood
count and group
and save sent
·
a urethral catheter should be inserted
·
the
baby should be delivered within
a maximum 30 min after
the decision

Related Topics