Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Absent Periods
ABSENT PERIODS
History
An
18-year-old woman presents
with an absence of periods
for 6 months. This has occurred twice before in the past but on both occasions menstruation returned so she was not
too concerned. Her periods started
at the age of 12 years and were initially
regular. She has no medical history
of note and
denies any medication. She is currently in her first year at university. She runs most days and reports a ‘healthy’ diet avoiding carbohydrate foods and meat. She
is the oldest
of three siblings and her parents
separated when she
was 12 years. She
has minimal contact
with her father
and lives mainly
with her mother
who she says she gets on well with. She has had a boyfriend in the past but has veered away from any sexual relationships.
Examination
The
woman is tall
and thin with
a body mass
index (BMI) of 15.5 kg/m2.
There is evidence of fine downy hair growth on
her arms. Heart rate is 86/min and blood pressure 100/65 mmHg. Abdominal examination reveals no scars
or masses, and
genital examin- ation is not performed.
Questions
·
What is the diagnosis?
·
How
would you further
investigate and manage this woman?
Answer:
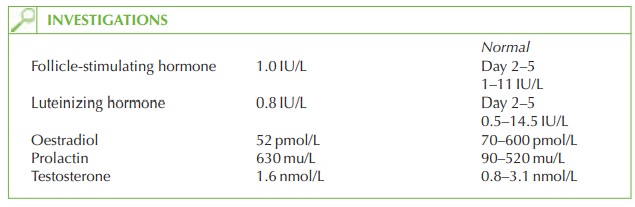
The
woman has evidence
of hypogonadotrophic hypogonadism – she has low oestradiol levels associated with low gonadotrophin stimulation from the anterior
pituitary. This may be due to various pituitary or hypothalamic causes,
but in this
case clearly relates
to anorexia nervosa and
possibly excessive exercise. The raised prolactin is consistent with stress and does not need to be investigated further. At a BMI below
18 kg/m2, menstru- ation tends to cease, returning once the BMI increases again.
The
previous episodes of amenorrhoea probably
occurred when her dietary intake was
very low and it may be that starting at university may have increased her stress levels with the consequence of worsening her anorexia.
Further investigation
·
Full blood count, liver
and renal function
should all be monitored as these are affected in severe disease.
·
A
bone scan should
be arranged to check for
bone density – hypo-oestrogenism as a
result of anorexia is likely
to induce early-onset osteoporosis and fractures.
·
Pyschological assessment is also
important to guide
appropriate treatment.
Management
Encouraging the woman to eat a more normal
diet and to avoid exercising is the ideal management, but anorexia is a chronic
disease that is often refractory to treatment.
Explanation that her periods will return if she increases her BMI may possibly encourage her to put on weight.
The
combined oral contraceptive pill should be prescribed in the meantime,
which will prevent osteoporosis and bring on periods, albeit
pharmacologically induced.
Referral to a specialist eating disorders unit is vital
in addressing the long-term problem for this woman. Commonly, eating disorders arise
out of childhood difficulties and family
or group therapy should be considered.
If
the investigations suggest
renal or hepatic
impairment then inpatient management is likely
to be necessary.
Related Topics