Chapter: Obstetrics and Gynecology: The Woman’s Health Examination
Bimanual Examination
BIMANUAL EXAMINATION
The bimanual examination uses both a
“vaginal” hand and an “abdominal” hand to entrap and palpate the pelvic organs.
The bimanual examination begins by
exerting gentle pres-sure on the abdomen approximately halfway between the
umbilicus and the pubic hair line with the abdominal hand, while inserting the
index and middle fingers of the vaginal hand into the vagina to approximately 2
inches and gently pushing downward, distending the vaginal canal. The pa-tient
is asked to feel the muscles being pushed on and to relax them as much as
possible. Then both the index and middle fingers are inserted into the vagina
until they rest at the limit of the vaginal vault in the posterior fornix
behind and below the cervix. A great deal of space may be created by posterior
distension of the perineum. Occasionally, only the index finger of the vaginal
hand can be comfort-ably inserted.
During the bimanual examination, the
pelvic struc-tures are “caught” and palpated between the abdominal and vaginal
hands. Whether to use the dominant hand as the abdominal or vaginal hand is a
question of personal preference. A common
error in this part of the pelvic examina-tion is failure to make effective use
of the abdominal hand. Pressure should be applied with the flat part of the
fingers, not the fingertips, starting midway between the umbilicus and the
hairline, moving downward in conjunction with upward movements of the vaginal hand.
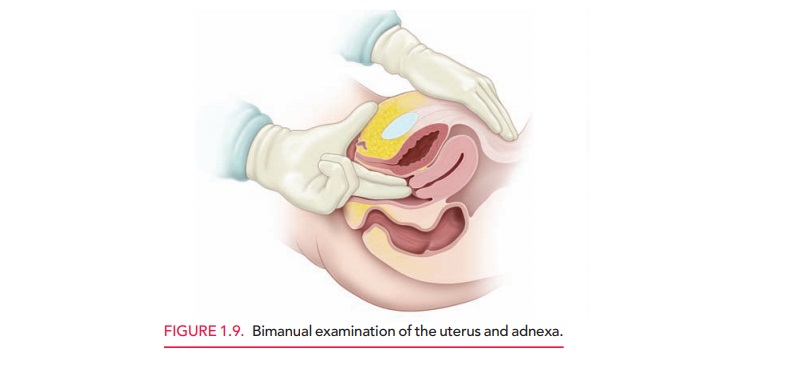
The bimanual ex-amination continues with the circumferential examination of the
cervix for its size, shape, position, mobility, and the presence or absence of
tenderness or mass lesions (Fig. 1.9).
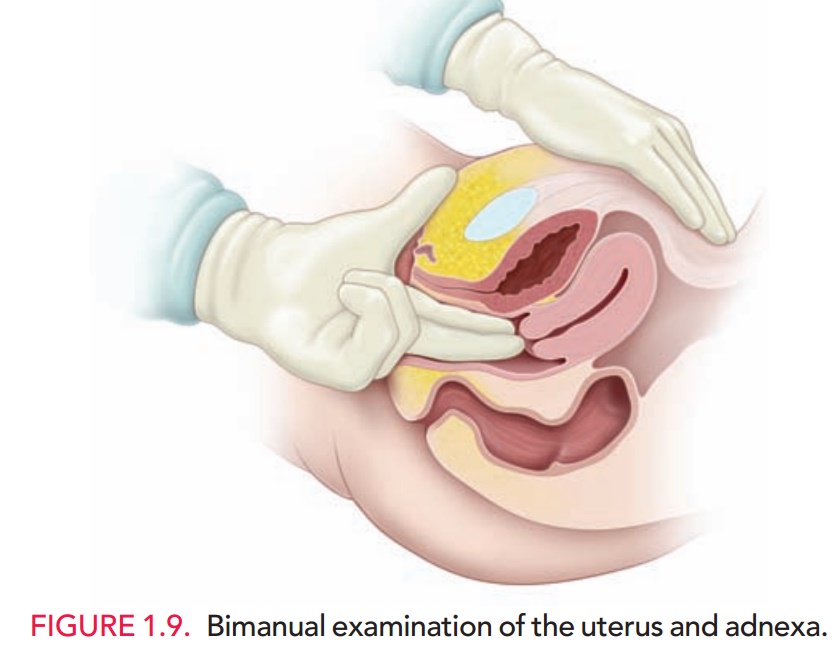
Bimanual examination of the uterus is accomplishedby lifting the uterus up toward the abdominal fingers so that it may be palpated between the vaginal and abdominal hands. The uterus is evaluated for its size, shape, consis-tency, configuration, and mobility; for masses or tenderness; and for position. The uterus may tilt on its long axis (from cervix to fundus, version) yielding three positions (ante-verted, midposition, and retroverted). It may also tilt ona shorter axis (from just above or at the area of the lower uterine segment, flexion) yielding two positions (ante-flexed and retroflexed) (see Fig. 4-12). The retroverted,retroflexed uterus has three particular clinical associations:
it is especially difficult to
estimate gestational age by bi-manual examination, (2) it is associated with
dyspareunia and dysmenorrhea, and (3) its position behind and below the sacral
promontory may lead to the obstetric complica-tion of uterine inculcation. Cervical
positionis often relatedto
uterine position. A posterior cervix is often associated with an anteverted or
midposition uterus, whereas an anterior cervix is often associated with a
retroverted uterus. Sharp flexion of theuterus, however, may alter these
relations.
The
bimanual examination technique varies somewhat with the position of the uterus.
Examination of the anterior and mid-position uterus
is facilitated with the vaginal fingers lateral and deep to the cervix in the
posterior fornix. The uterus is gently lifted upward to the abdominal fingers
and a gentle side-to-side “searching” motion of the vaginal fingers is combined
with steady pressure and palpation by the abdom-inal hand to determine the
characteristics of the uterus.
Examination of the retroverted
uterus may be more difficult. In some cases, the vaginal fingers may be slowly
pushed below or at the level of the uterine fundus, after which gentle pressure
exerted inward and upward causes the uterus to antevert, or at least to move
“upward,” some-what facilitating palpation. Then palpation is accomplished as
in the normally anteverted uterus. If this cannot be done, a waving motion with
the vaginal fingers in the posterior fornix must be combined with an extensive
rectovaginal examination to assess the retroverted uterus.
Bimanual
examination of the adnexa to assess theovaries, fallopian
tubes, and support structures begins by placing the vaginal fingers to the side
of the cervix, deep in the lateral fornix. The abdominal hand is moved to the
same side, just inside the flare of the sacral arch and above the pubic
hairline. Pressure is then applied downward and toward the symphysis with the
abdominal hand, at the same time lifting upward with the vaginal fingers. The
same movements of the fingers of both hands used to as-sess the uterus are used
to assess the adnexal structures, which are brought between the fingers by
these maneu-vers to evaluate their size, shape, consistency, configuration,
mobility, and tenderness, as well as to palpate for masses. Special care must be taken when examining
the ovaries, which are sensitive even in the absence of pathology. The ovaries
are palpable in normal menstrual women approximately half of the time, whereas
palpation of ovaries in postmenopausal women is less common.
Related Topics