Chapter: Obstetrics and Gynecology: Disorders of the Breast
Benign Breast Disease
BENIGN BREAST DISEASE
Benign
breast disease includes a large number of condi-tions that can
significantly affect a woman’s quality of life. With accurate diagnosis, many
benign breast conditions can be effectively treated with medications or other
mea-sures. Women presenting with a breast mass should also be evaluated for
their risk of breast cancer.
Mastalgia
Mastalgia, or breast pain, can be divided
into three categories:cyclic, noncyclic, and extramammary (nonbreast) pain. Cyclicmastalgia begins
with the luteal phase of the menstrualcycle and resolves after the onset of
menses. The pain is generally bilateral and often involves the upper outer
quadrants of the breast. Noncyclic
mastalgia is not associated with the menstrual cycle and includes such
eti-ologies as tumors, mastitis, cysts, and a history of breast surgery. In
some women, noncyclic mastalgia is idiopathic and no cause is found. Noncyclic
pain has also been associ-ated with some medications, including hormonal
medica-tions, antidepressants such as sertraline and amitriptyline, and
antihypertensive drugs, in addition to others. If the onset of mastalgia is
associated with the start of hormonal therapy, stopping or reducing the
hormones may be ben-eficial. Nonmammary
pain can be caused by a number of conditions, such as chest wall trauma,
rib fractures, and fibromyalgia. Treatment for musculoskeletal disorders
includes antiinflammatory drugs, but more serious causes of chest pain, such as
angina, need to be ruled out.
The only
medication approved by the FDA for treat-ing mastalgia is danazol, but it has
significant side effects. Other hormonal therapies that may
decrease pain include bromocriptine and gonadotropin-releasing hormone
ago-nists, but these drugs also have side effects that limit their widespread
use. Lisuride maleate is a dopamine agonist that has shown pain-reducing
effects, and it has fewer side effects than bromocriptine. Selective estrogen receptor modula-tors, such as tamoxifen, also have a
role in treating severe mastal-gia. These medications act as estrogen
antagonists in thebreast. Side effects of tamoxifen include an increased risk
of endometrial hyperplasia and deep venous thrombosis, as well as hot flushes
and vaginal bleeding. A recent study concluded that side effects are reduced
when the medica-tion is given in smaller doses.
Tamoxifen
should be used only for cases of severe mastalgia that does not respond to
other therapies.
Some women with cyclic mastalgia
have reported a decrease in pain with oral contraceptives or the injectable
contraceptive medroxyprogesterone acetate.
Nonpharmacologic measures to help
relieve breast pain include a properly fitting brassiere or a sports bra worn
throughout the day or during exercise, weight reduction, and regular exercise.
Although no studies have demon-strated the efficacy of these measures, they are
worth recommending to patients and may help relieve pain.
Nipple Discharge
Nipple discharge is usually
benign, but may be an early sign of endocrine dysfunction or cancer. The color,
consistency, and whether the discharge is bilateral or unilateral can yield
important clues about its cause. A nonspontaneous, non-bloody, bilateral nipple
discharge is usually attributed to fibrocystic changes of the breast or ductal ectasia, a con-dition
characterized by dilation of the mammary ducts, periductal fibrosis, and
inflammation. Ductal ectasia is seen in adolescent women as well as in
perimenopausal women. Milky discharge is common during childbearing, but it can
also be associated with other endocrinologic abnormalities (hyperprolactinemia
or hypothyroidism) and medications (oral contraceptives and tricyclic
anti-depressants). Purulent discharge may indicate an infectious etiology and
may be due to mastitis or a breast abscess. Green, yellow, or brown sticky
discharge can be due to duc-tal ectasia or fibrocystic changes of the breast.
Bloody, unilateral nipple
discharge may be caused by an invasive ductal carcinoma, intraductal papilloma,
or an intraductal carcinoma. Patients with nipple discharge of this type
usually require ductography and ductal excision. Breast ductography is an
imaging technique that can reveal the location of an intraductal lesion. A new technique thatemploys fiberoptic
technology, fiberoptic ductoscopy (FDS), allows the direct visualization of the
breast ducts, as well as sampling of ductal cells. However, this modality
is not widely available.
Breast Masses
The most worrisome finding for
patients and clinicians is an unexplained breast mass. Some characteristics of
breast masses that suggest malignancy include size greater than 2 cm,
immobility, poorly defined margins, firmness, skin dimpling or color changes,
retraction or change in the nipple (e.g., scaling), bloody nipple discharge,
and ipsilat-eral lymphadenopathy. The growth rate of a tumor in the breast is
thought to be constant from the time of its ori-gin. It is estimated that it
takes an average of 5 years for a tumor to reach palpable size.
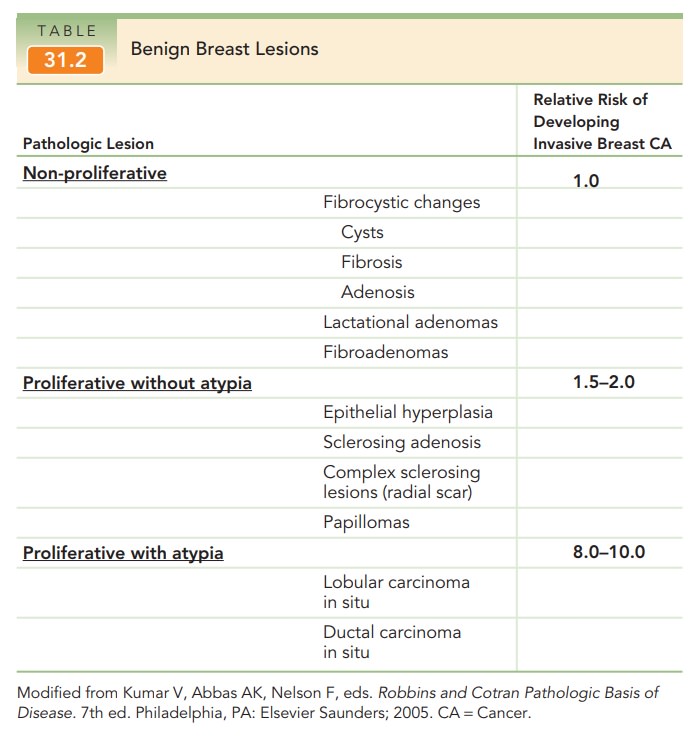
Benign Breast Masses
A variety of benign breast masses
are found on screening mammograms or incidentally. Table 31.2 summarizes the
three morphologic categories and their associated risk of developing invasive
breast cancer.
NON-PROLIFERATIVE LESIONS
Fibrocystic changes of the breast
are a
spectrum of featuresthat can be observed in the normal breast. Lobules
of thebreast may dilate and form cysts of varying sizes. The cyst walls are
lined by flattened atrophic epithelium or may be modified through apocrine
metaplasia. If these cysts rup-ture, the resulting scarring and inflammation
may lead to fibrotic changes which make the breast feel firm. An increase in
the number of glands with associated lobular growth is known as adenosis. In this case, the
architecture of the lobule remains unchanged. In some lactating women, a
palpable lactation adenoma may arise secondary to an exaggerated hormonal
response.
Simple fibroadenomas are common tumors found inwomen in their late teens and early twenties. These masses are solid, round, rubbery, and mobile on examination.
The tumors do have structural and
glandular components in the mass. Although they do not have malignant
poten-tial, they can enlarge in pregnancy and cause discomfort.
PROLIFERATIVE LESIONS WITHOUT ATYPIA
These lesions are commonly found
on mammography and do not usually cause a palpable mass. Histologically, they
represent proliferation of cells of the ductal or lobular epithelium. The cells
themselves are normal, i.e., nonmalignant.
In a normal breast, only myoepithelial cells and a single layer of luminal cells rest on the basement. If there are more than 2 cell layers, the abnormality is known as epithelial hyperplasia. If there is increased fibrosiswithin the expanded lobule, with distortion and compres-sion of the epithelium, the lesion is termed sclerosingadenosis. A radial scar (or complex sclerosing lesion) is anidus of tubules entrapped in a densely hyalinized stroma surrounded by radiating arms of epithelium. The lesion mimics an invasive carcinoma. Finally, papillomas are intraductal growths composed of abundant stroma and lined by both luminal and myoepithelial cells. Solitary intraductal papillomas are found in the major lactiferous ducts of women, typically between the ages of 30 and 50, and cause a serous or serosanguineous drainage.
PROLIFERATIVE LESIONS WITH ATYPIA
When
malignant cells replace the normal epithelium lining the ducts or lobules, the
lesion is known as a carcinoma in situ. The
basement membrane remains intact and, therefore, the cells cannot metastasize.
There are two major types of
carcinoma in situ: lob-ular carcinoma in
situ (LCIS) and ductal carcinoma in
situ (DCIS). LCIS is characterized by obliteration of thelumina of the
glandular acini by a uniform population of small, atypical cells. In DCIS, the
ducts are filled with atyp-ical epithelial cells. Women with DCIS are at
increased risk of developing invasive cancer or a recurrence of the DCIS
lesion. For these reasons, DCIS should be evaluated with core-needle biopsy
followed by surgical biopsy or excision. Management of LCIS and its related
condition, atypical lobular hyperplasia, consists of excisional biopsy. Following treatment of both LCIS and DCIS,
preventive ther-apy with selective estrogen receptor modulators such as
tamox-ifen has been shown to reduce the risk of invasive breast cancer in these
patients.
Related Topics