Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Hearing and Balance Disorders
Aural Rehabilitation
Aural Rehabilitation
If hearing loss is permanent or cannot be treated
by medical or surgical means or if the patient elects not to undergo surgery,
aural rehabilitation may be beneficial. The purpose of aural re-habilitation is
to maximize the hearing-impaired person’s com-munication skills. Aural
rehabilitation includes auditory training, speech reading, speech training, and
the use of hearing aids and hearing guide dogs.
Auditory training emphasizes listening skills, so
the hearing-impaired person concentrates on the speaker. Speech reading
(formerly known as lip reading) can help fill the gaps left by missed or
misheard words. Speech training attempts to conserve, develop, and prevent
deterioration of current skills.
It is important to identify the type of hearing
impairment a person has so that rehabilitative efforts can be directed at his
or her particular need. Surgical correction may be all that is necessary to
treat and improve a conductive hearing loss (Fig. 59-10). With ad-vances in
hearing aid technology, amplification for patients with sensorineural hearing
loss is more helpful than ever before.
HEARING AIDS
A
hearing aid is a device through which speech and environmen-tal sounds are
received by a microphone, converted to electrical signals, amplified, and
reconverted to acoustic signals. Many aids available for sensorineural hearing
loss depress the low frequen-cies, or tones, and enhance hearing for the high
frequencies. A general guideline for assessing the patient’s need for a hearing
aid is a hearing loss exceeding 30 dB in the range of 500 to 2000 Hz in the
better-hearing ear.
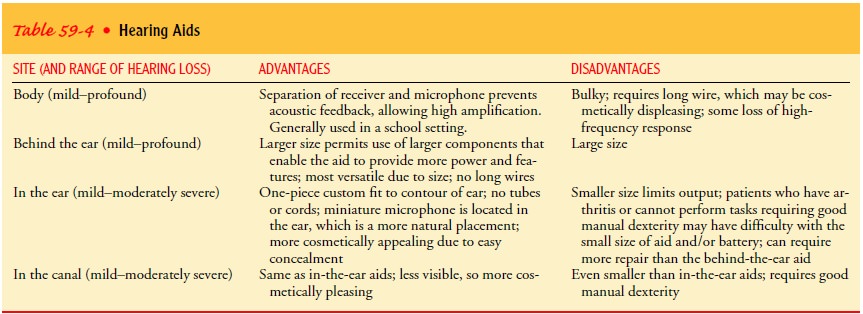
The
evolution in technology has led to the availability of many smaller and more
effective hearing aids. It is estimated that 98% of all hearing aids sold today
are behind-the-ear, in-the-ear, or in-the-canal types (Table 59-4).
A hearing aid should be fitted according to the patient’s needs (eg, type of hearing loss, manual dexterity), rather than the brand name, by a certified audiologist licensed to dispense hearing aids. Many states have a consumer protection law that allows the hear-ing aid to be returned after a trial use if the patient is not com-pletely satisfied.
A hearing aid makes sounds louder, but it does not improve a patient’s ability to discriminate words or understand speech. People who have low discrimination scores (ie, 20%) on audiograms may derive little benefit from a hearing aid. Hearing aids amplify all sounds, including background noise, which may be disturbing to the wearer. Chart 59-7 identifies additional problems associated with hearing aid use.

There are, however, computerized hearing aids available that compensate for background noise or allow amplification at certain programmed frequencies
rather than at all frequencies. Occasionally, depending on the type of hearing
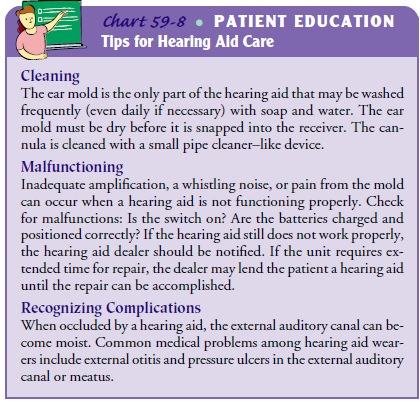
loss, binaural aids (ie, one for each ear) may be indicated. Chart 59-8
provides tips for hearing aid care.
To protect the health and safety of people with hearing impair-ments, the U.S. Food and Drug Administration (FDA) has estab-lished certain regulations. A medical evaluation of the impairment by a licensed physician must be obtained within 6 months before the purchase of a hearing aid. The written statement from a phy-sician may be waived, however, if the patient (a fully informed adult 18 years of age or older) signs a document to this effect.
Children
must be evaluated by a physician. Health care profes-sionals who dispense
hearing aids are required to refer prospec-tive users to a physician if any of
the following otologic conditions are evident:
·
Visible congenital or
traumatic deformity of the ear
·
Active drainage from the ear
within the previous 90 days
·
Sudden or rapidly progressive
hearing loss within the previ-ous 90 days
·
Complaints of dizziness or
tinnitus
·
Unilateral hearing loss that
occurred suddenly or within the previous 90 days
·
Audiometric air–bone gap of 15
dB or more at 500, 1000, and 2000 Hz
·
Significant accumulation of
cerumen or a foreign body in the external auditory canal
·
Pain or discomfort in the ear
A user instruction brochure is to accompany every
hearing aid device. In this brochure, the following information is presented:
·
Specification that good health
practice requires a medical evaluation before purchasing a hearing aid
·
Notification that any of the
eight otologic conditions pre-viously listed should be investigated by a
physician before purchase of a hearing aid
·
Instructions for proper use,
maintenance, and care of the hearing aid, as well as instructions for replacing
or recharg-ing the batteries
·
Repair service information
·
Description of avoidable
conditions that could damage the hearing aid
·
List of any known side effects
that may warrant physician consultation (eg, skin irritation, accelerated
cerumen accu-mulation)
IMPLANTED HEARING DEVICES
Three types of implanted hearing devices are
commercially avail-able or in the investigational stage: the cochlear implant,
the bone conduction device, and the semi-implantable hearing device. Cochlear
implants are for patients with little or no hearing. Bone conduction devices,
which transmit sound through the skull to the inner ear, are used in patients
with a conductive hearing loss if a hearing aid is contraindicated (eg, those
with chronic infec-tion). The device is implanted postauricularly under the
skin into the skull, and an external device—worn above the ear, not in the
canal—transmits the sound through the skin. Semi-implantable hearing aids,
although not yet approved by the FDA except in testing sites, still require the
use of an external device. However, research to develop a fully implantable
hearing aid continues.
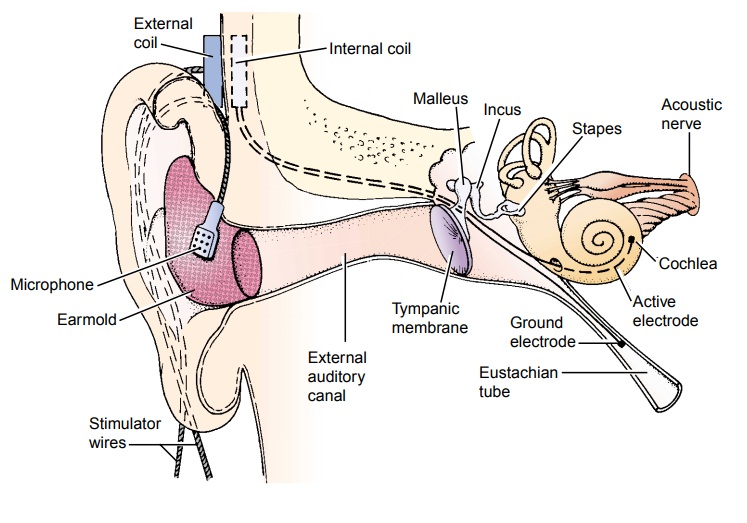
Cochlear Implant
A cochlear implant is an auditory prosthesis used for people with profound sensorineural hearing loss bilaterally who do not bene-fit from conventional hearing aids. The hearing loss may be con-genital or acquired. An implant does not restore normal hearing; rather, it helps the person detect medium to loud environmental sounds and conversation. The implant is designed to provide stimulation directly to the auditory nerve, bypassing the hair cells of the inner ear, which are not functioning. The microphone and signal processor are worn outside the body and transmit electri-cal stimuli inside the body to the implanted electrodes. The elec-trical signals stimulate the auditory nerve fibers and then the brain, where they are interpreted.
Candidates
for a cochlear implant, who are usually at least 1 year old, are selected after
careful screening by otologic history, physical examination, audiologic
testing, x-rays, and psychologi-cal testing. Several criteria apply for
choosing adults who may ben-efit from a cochlear implant:
·
Profound sensorineural hearing
loss in both ears
·
Inability to hear and
recognize speech well with hearing aids
·
No medical contraindication to
a cochlear implant or gen-eral anesthesia
·
Indications that being able to
hear would enhance the patient’s life
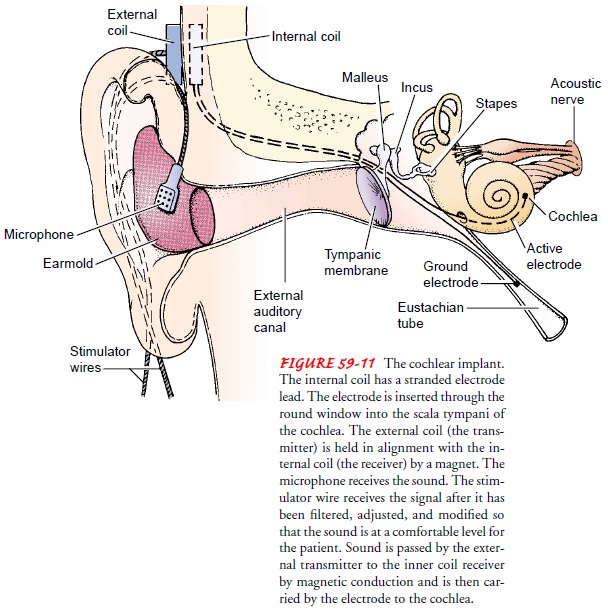
The surgery involves implanting a small receiver in
the tempo-ral bone through a postauricular incision and placing electrodes into
the inner ear (Fig. 59-11). The microphone and transmitter are worn on an
external unit. The patient undergoes extensive cochlear rehabilitation with the
multidisciplinary team, which includes an audiologist and speech pathologist.
Several months may be needed to learn to interpret the sounds heard. Children
and adults who lost their hearing before they learned to speak take much longer
to ac-quire speech. There are wide variations of success with cochlear
im-plants, and there is also controversy about their use, especially among the
Deaf community. Patients who have had a cochlear im-plant are cautioned that an
MRI will cause the implant to become inactivated; MRI is to be used only when
unavoidable.
HEARING GUIDE DOGS
Specially trained dogs are available to assist the
person with a hear-ing loss. People who live alone are eligible to apply for a
dog trained by International Hearing Dog, Inc. At home, the dog reacts to the
sound of a telephone, a doorbell, an alarm clock, a baby’s cry, a knock at the
door, a smoke alarm, or an intruder. The dog does not bark but alerts its
master by physical contact; the dog then runs to the source of the noise. In
public, the dog positions itself between the hearing-impaired person and any
potential hazard that the per-son cannot hear, such as an oncoming vehicle or a
loud, hostile per-son. In many states, a hearing-impaired person with a
certified hearing guide dog is legally permitted access to public
transporta-tion, public eating places, and stores, including food markets.
Related Topics