Chapter: Modern Medical Toxicology: General Principles: General Management of Poisoning
Antidote Administration - General Management of Poisoning
Antidote Administration
In
the majority of cases of acute poisoning, all that is required is intensive
supportive therapy with attention to all the details mentioned in the preceding
sections. Specific antidotes are rarely necessary, besides the fact that only a
few genuine antidotes exist in actual practice, though there is no denying the
dramatic results that can be achieved with some of them in appropriate
circumstances. Proper antidotal therapy can be life-saving in some situations.
Antidotes
work in any one of a number of ways. Common modes of action are as follows:
Inert complex formation
Some
antidotes interact with the poison to form an inert complex which is then
excreted from the body, e.g. chelating agents for heavy metals, Prussian Blue
for thallium, specific antibody fragments for digoxin, dicobalt edetate for
cyanide, etc.
Accelerated detoxification
Some
antidotes accelerate the detoxification of a poison,e.g. thiosulfate
accelerates the conversion of cyanide to non-toxic thiocyanate, acetylcysteine
acts as a glutathione substitute which combines with hepatotoxic paracetamol
metabolites and detoxifies them.
Reduced toxic conversion
The
best example of this mode of action is provided by ethanol which inhibits the
metabolism of methanol to toxic metabolites by competing for the same enzyme
(alcohol dehy-drogenase).
Receptor site competition Some antidotes displace the poison
from specific receptor sites, thereby antagonising the effects completely. The
best example is provided by naloxone, which antagonises the effects of opiates
at stereo-specific opioid receptor sites.
Receptor site blockade
This mode of action is best
exemplified by atropine which blocks the effects of anticholinesterase agents
such as organo-phosphates at muscarinic receptor sites.
Toxic effect bypass
An example of this type of antidotal
action is provided by the use of 100% oxygen in cyanide poisoning.
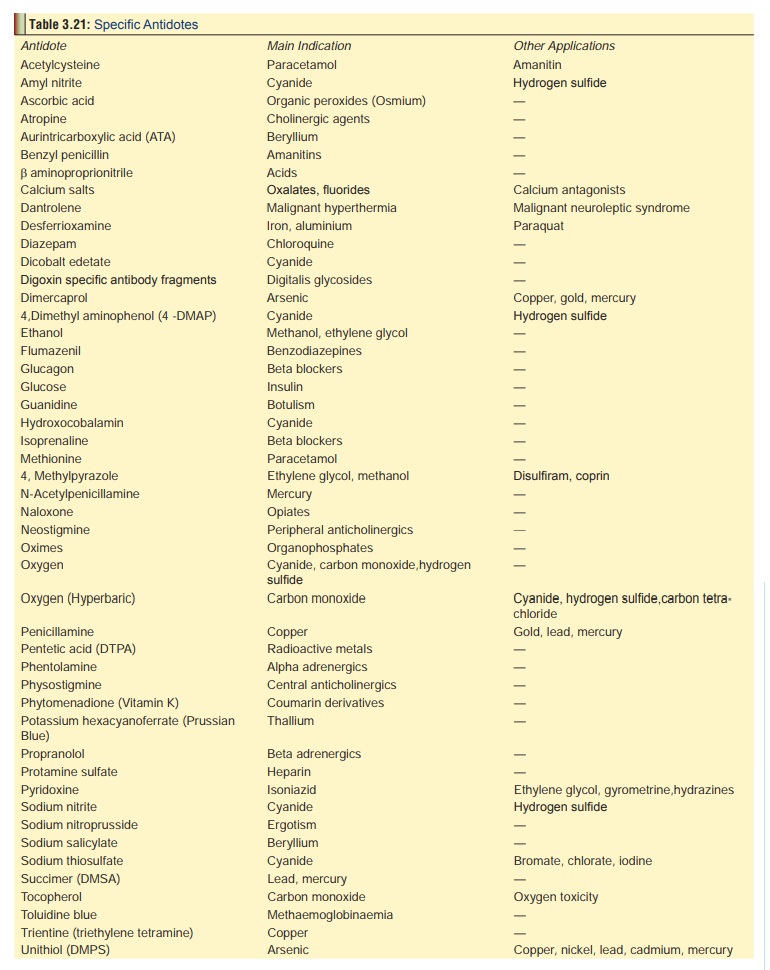
Table 3.21 represents a list of genuine antidotes recom-mended in
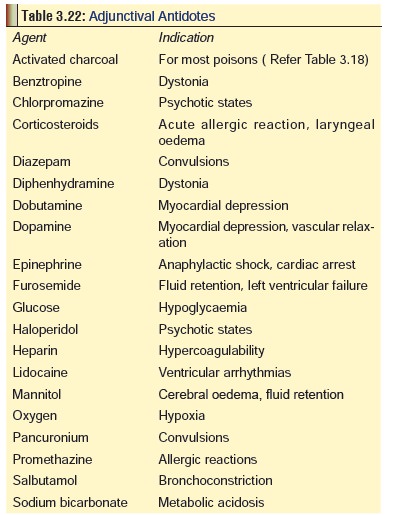
toxicological practice today. In addition, there are certain therapeutic agents
which are not antidotes as per the accepted definition, but which through their
importance and sometimes specific role in the treatment of poisons, border on
the concept of “antidotes”. Table 3.22
represents a list of such substances. Unfortunately in India, cumbersome
governmental regulations and a lack of economic incentives for manufacturers
have restricted availability of a substantial number of these life-saving
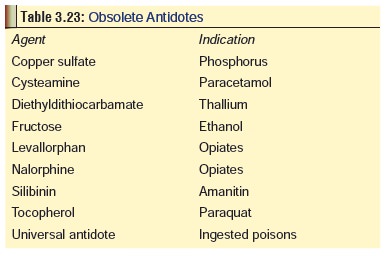
drugs. As a result, doctors still use some substances which are more readily
available as antidotes, but are generally considered obsolete or even dangerous
in Western countries (Table 3.23).
It is imperative that medical professionals strive to phase out these obsolete
drugs, while working out strategies to make genuine antidotes more readily
available.
Related Topics