Chapter: Biology of Disease: Disorders of the Cardiovascular System
Angina - Atherosclerosis or Arteriosclerosis
ANGINA
Angina pectoris is caused by myocardial ischemia. It
presents as a crushing or squeezing pain in the chest and the discomfort may
radiate into the neck, jaw, arms (especially the left) and sometimes into the
back. There may also be shortness of breath, abdominal pain, nausea and
dizziness. Myocardial oxygen demand relates to the heart rate, left ventricular
contractility and systolic wall stress. The demand for oxygen is increased by
exercise, hypertension and left ventricular dilation, which may happen in
chronic heart failure.
Several types of angina are recognized. Stable angina
occurs when atherosclerotic plaques block one or more of the coronary arteries.
Under resting conditions, cardiac oxygen demand is quite low and is satisfied
even by the diminished blood flow. However, when exertion or emotional stresses
increase this oxygen demand, ischemia develops on the inner part of the
myocardial wall. However, the response to exercise is variable: some patients
may have excellent exercise tolerance one day and then develop angina with
minimal exertion the next. In addition to causing pain, the ischemia causes a
decline in the output of ATP and creatine phosphate and hence contractility is impaired.
Stable angina is normally relieved by a short rest or by administering glyceryltrinitrate.
The latter dilates the arteries, increasing blood, and therefore oxygen,
supplies to the muscle leading to less pain.
Variant angina is an intensely painful, transient
spasm caused by a blockage of one of the coronary arteries. It is relatively
uncommon, but can occur at rest. It is exacerbated by smoking and by cocaine
use. About one-third of patients show no evidence of atherosclerotic lesions.
Ischemic heart disease and stable angina can be
distinguished from other conditions that cause chest pain on the basis of their
characteristic symptoms and by a number of types of diagnostic tests, for
example the ECG, exercise stress test and by using coronary angiography to
obtain a direct radiographic visualization, as described earlier.
The management of angina is designed to control the
symptoms and reduce any underlying risk factors. The drugs used include the
nitrovasodilators, for example glyceryltrinitrate, A-adrenoceptor blockers, calcium
channel antagonists, as well as drugs that inhibit platelet aggregation and
thrombosis. In the case of stable angina, mortality is 2 to 4% a year if only
one coronary artery is diseased but increases with the number of diseased
arteries.
The other main variant of angina is the so-called
unstable angina, which is a dangerous condition, often heralding an impending
myocardial infarction. In general, the symptoms resemble those of stable angina
but are more intense and persistent, often lasting 30 min, and the pain is
often resistant to glyceryltrinitrate treatment. The attacks may be frequent,
becoming progressively more severe and prolonged, may be brought on by minimal
exertion (or even during sleep) or may occur several days after a myocardial
infarction. The episodes are preceded by a fall in coronary blood flow, which
is thought to be the result of the periodic development of coronary thrombosis
and vasoconstriction. These are triggered by coronary arterial disease. The
thrombosis may be promoted by the turbulent blood flow associated with atherosclerotic
plaques: there may also be damage to the endothelial lining of the blood
vessels.
An ECG is taken to help in the diagnosis but, in
addition, serum levels of C-reactive protein and amyloid-A protein may be
increased; these are classic markers of inflammation. Unstable angina is a
medical emergency and treatment usually begins with aggressive drug therapy to
control the symptoms and prevent further episodes, and to try to reverse
coronary vasospasm. Platelet glycoproteins IIIA and IIb (Tirofiban and ReoPro)
are now used in unstable angina to stabilize the clot in the narrowed coronary
artery, which is causing the pain, prior to angiography and possibly
angioplasty and stenting. Angioplasty is a procedure similar to angiography but
the catheter delivers a small inflatable balloon to the narrowed portion of the
coronary artery. When the balloon is inflated it opens the restricted section
of the artery. Stents are very small, coated spring-like structures that are
deployed, by cardiac catheters into the narrowed section following angioplasty.
They act like miniature struts to maintain the opening of the vessel.
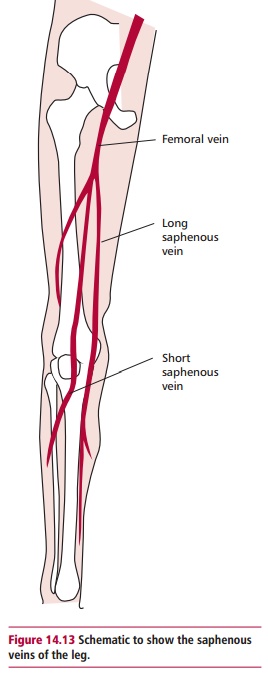
Urgent revascularization needs to be considered for
patients at high risk, or unsuitable for angioplasty/stenting due to
significant coronary arterial disease. In a coronary artery bypass grafting a
length of healthy ‘surplus’ blood vessel, such as the saphenous vein from the
leg (Figure 14.13), is obtained and
pieces of it are inserted between the aorta and the coronary arteries distal to
any stenosis (narrowing). The left internal mammary artery may also be used. A
bypass improves survival in patients with severe atherosclerotic disease in all
the major coronary arteries.
Related Topics