Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Anesthetic Complications
Anesthetic Complications: Pediatric Anesthesia
PEDIATRIC ANESTHESIA
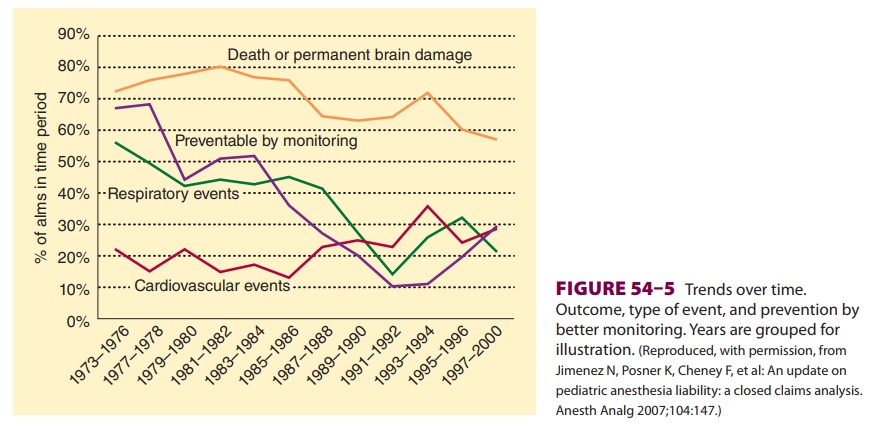
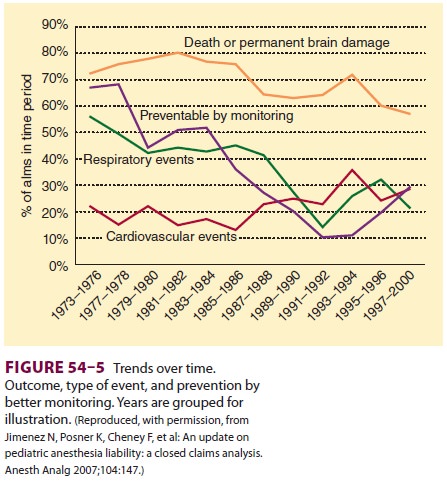
In a 2007 study reviewing 532 claims in
pediatric patients aged <16 years in the ASA Closed Claims database from 1973–2000 (Figure
54–5), a decrease in the proportion of claims for
death and brain dam-age was noted over the three decades. Likewise, the
percentage of claims related to respiratory events also was reduced. Compared
with before 1990, the percentage of claims secondary to respiratory events
decreased during the years 1990–2000, account-ing for only 23 % of claims in
the latter study years compared with 51% of claims in the 1970s. More-over, the
percentage of claims that could be avoided by better monitoring decreased from
63% in the 1970s to 16% in the 1990s. Death and brain dam-age constitute the
major complications for which claims are filed. In the 1990s, cardiovascular
events joined respiratory complications in sharing the pri-mary causes of
pediatric anesthesia litigation. In the study mentioned above, better
monitoring and newer airway management techniques may have reduced the
incidence of respiratory events leading to litigation-generating complications
in the latter years of the review period. Additionally, the possi-bility of a
claim being filed secondary to death or brain injury is greater in children who
are in ASA classes 3, 4, or 5.
In a review of the Pediatric Perioperative
Cardiac Arrest Registry, which collects informa-tion from about 80 North
American institutions that provide pediatric anesthesia, 193 arrests were
reported in children between 1998 and 2004. Dur-ing the study period, 18% of
the arrests were “drug related,” compared with 37% of all arrests during the
years 1994–1997. Cardiovascular arrests occurred most often (41%), with
hypovolemia and hyperka-lemia being the most common causes. Respiratory arrests
(27%) were most commonly associated with laryngospasm. Central venous catheter placement
with resultant vascular injury also contributed to some perioperative arrests.
Arrests from cardio-vascular causes occurred most frequently during surgery,
whereas arrests from respiratory causes tended to occur after surgery. The
reduced use of halothane seems to have decreased the incidence of arrests
secondary to medication administration. However, hyperkalemia and electrolyte
disturbances
associated with transfusion and hypovolemia also contribute to sources
of cardiovascular arrest in chil-dren perioperatively.
review of data from the Pediatric
Periopera-tive Cardiac Arrest Registry with a focus on chil-dren with
congenital heart disease found that such children were more likely to arrest
perioperatively secondary to a cardiovascular cause. In particular, children
with a single ventricle were at increased risk of perioperative arrest.
Children with aortic stenosis and cardiomyopathy were similarly found to be at
increased risk of cardiac arrest perioperatively.
Related Topics