Chapter: Clinical Anesthesiology: Clinical Pharmacology: Adjuncts to Anesthesia
5 HT3 Receptor Antagonists
5 HT3 RECEPTOR ANTAGONISTS
Serotonin Physiology
Serotonin,
5-hydroxytryptamine (5-HT), is present in large quantities in platelets and the
GI tract (entero-chromaffin cells and the myenteric plexus). It is also an
important neurotransmitter in multiple areas of the central nervous system.
Serotonin is formed by hydroxylation and decarboxylation of tryptophan.
Monoamine oxidase inactivates serotonin into 5-hydroxyindoleacetic acid
(5-HIAA). The physiol-ogy of serotonin is very complex because there are at
least seven receptor types, most with multiple sub-types. The 5-HT3
receptor mediates vomiting and is found in the GI tract and the brain (area
postrema). The 5-HT2A receptors are responsible for smooth muscle
contraction and platelet aggregation, the 5-HT4 receptors in the GI
tract mediate secretion and peristalsis, and the 5-HT6 and 5-HT7
receptors are located primarily in the limbic system where they appear to play
a role in depression. All except the 5-HT3 receptor are coupled to G
proteins and affect either adenylyl cyclase or phospholipase C; effects of the
5-HT3 receptor are mediated via an ion channel.
A. Cardiovascular
Except in the heart and skeletal muscle,
serotonin is a powerful vasoconstrictor of arterioles and veins. Its
vasodilator effect in the heart is endotheliumdependent. When the myocardial
endothelium is damaged following injury, serotonin produces vaso-constriction.
The pulmonary and renal vasculatures are very sensitive to the arterial
vasoconstrictive effects of serotonin. Modest and transient increases in
cardiac contractility and heart rate may occur immediately following serotonin
release; reflex bra-dycardia often follows. Vasodilation in skeletal mus-cle
can subsequently cause hypotension.
B. Respiratory
Contraction of smooth muscle increases
airway resistance. Bronchoconstriction from released sero-tonin is often a
prominent feature of carcinoid syndrome
C. Gastrointestinal
Direct
smooth muscle contraction (via 5-HT2 recep-tors) and
serotonin-induced release of acetylcholine in the myenteric plexus (via 5-HT3
receptors) greatly augment peristalsis. Secretions are unaffected.
D. Hematological
Activation
of 5-HT2 receptors causes platelet aggregation.
Mechanism of Action
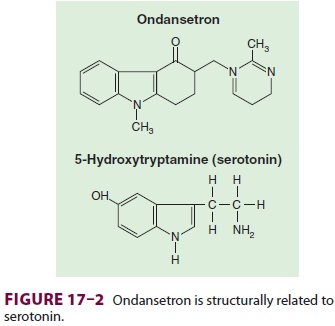
Ondansetron
(Zofran), granisetron (Kytril), and dolasetron (Anzemet) selectively
blockserotonin 5-HT3 receptors, with little or no effect on dopamine
receptors (Figure
17–2). 5-HT3
receptors,
which are located peripherally (abdomi-nal vagal afferents) and centrally
(chemoreceptor trigger zone of the area postrema and the nucleus tractus
solitarius), appear to play an important role in the initiation of the vomiting
reflex. The 5-HT3 receptors of the chemoreceptor trigger zone in the
area postrema reside outside the blood–brain bar-rier. The trigger zone is
activated by substances such as anesthetics and opioids and signals the nucleus
tractus solitarius, resulting in PONV. Emetogenic stimuli from the GI tract
similarly stimulate the development of PONV.
Clinical Uses
5-HT3-receptor
antagonists are generally admin-istered at the end of surgery. All these agents
are effective antiemetics in the postoperative period. In comparison with other
antiemetic agents such as droperidol (1.25 mg) and dexamethasone (4 mg),
ondansetron appears equally effective. A new agent, palonosetron (Aloxi), has
an extended duration of action and may reduce the incidence of postdis-charge
nausea and vomiting (PDNV).
Side Effects
5-HT3
receptor antagonists are essentially devoid of serious side effects, even in
amounts several times the recommended dose. They do not appear to cause
sedation, extrapyramidal signs, or respi-ratory depression. The most commonly
reported side effect is headache. All three drugs can slightly prolong the QT
interval on the electrocardiogram. This effect may be more frequent with
dolasetron, although it has not been associated with any adverse arrhythmias.
Nonetheless, these drugs, particularly dolasetron, should be used cautiously in
patients who are taking antiarrhythmic drugs or who have a prolonged QT
interval.
Ondansetron
undergoes extensive metabo-lism in the liver via hydroxylation and conjuga-tion
by cytochrome P-450 enzymes. Liver failure impairs clearance several-fold, and
the dose should be reduced accordingly. The recommended intrave-nous dose is
12.5 mg for dolasetron and 1 mg for granisetron. All three drugs are available
in oral for-mulations for PONV prophylaxis.
Related Topics